You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Trust Is The Coin of The Realm by George P. ShultzDocument13 pagesTrust Is The Coin of The Realm by George P. ShultzHoover Institution100% (2)
- ESSAYDocument1 pageESSAYJunalie GregoreNo ratings yet
- BK Hodd 000401Document25 pagesBK Hodd 000401KhinChoWin100% (1)
- How To Write A ThesisDocument14 pagesHow To Write A ThesisPiyushNo ratings yet
- Research Design1 USED 6Document14 pagesResearch Design1 USED 6Joselle RuizNo ratings yet
- Javier Guzman v. City of Cranston, 812 F.2d 24, 1st Cir. (1987)Document4 pagesJavier Guzman v. City of Cranston, 812 F.2d 24, 1st Cir. (1987)Scribd Government DocsNo ratings yet
- Precision Nutrition. Nutrient TimingDocument21 pagesPrecision Nutrition. Nutrient TimingPaolo AltoéNo ratings yet
- Study On Perfromance Appraisal System in HPCLDocument12 pagesStudy On Perfromance Appraisal System in HPCLomkinggNo ratings yet
- 2007 - Q1 NewsletterDocument20 pages2007 - Q1 NewsletterKisara YatiyawelaNo ratings yet
- Whats New PDFDocument74 pagesWhats New PDFDe Raghu Veer KNo ratings yet
- Kalki ProjectDocument3 pagesKalki ProjectMandar SohoniNo ratings yet
- Mcqmate Com Topic 333 Fundamentals of Ethics Set 1Document34 pagesMcqmate Com Topic 333 Fundamentals of Ethics Set 1Veena DeviNo ratings yet
- Notes in Ophthalmology: MCQ, Osce, SlidDocument21 pagesNotes in Ophthalmology: MCQ, Osce, SlidDrmhdh DrmhdhNo ratings yet
- The Utopia of The Zero-OptionDocument25 pagesThe Utopia of The Zero-Optiontamarapro50% (2)
- 10 Applications in Engineering Mechanics PDFDocument10 pages10 Applications in Engineering Mechanics PDFWolf Lord100% (1)
- 10 1108 - JKM 01 2020 0064Document23 pages10 1108 - JKM 01 2020 0064BBA THESISNo ratings yet
- 17373.selected Works in Bioinformatics by Xuhua Xia PDFDocument190 pages17373.selected Works in Bioinformatics by Xuhua Xia PDFJesus M. RuizNo ratings yet
- Boado Notes On Criminal LawDocument55 pagesBoado Notes On Criminal LawJoy100% (3)
- MarshallingDocument7 pagesMarshallinggeetika singhNo ratings yet
- Business Finance Chapter 4Document15 pagesBusiness Finance Chapter 4chloe frostNo ratings yet
- FASUPDocument60 pagesFASUPPranjal KumarNo ratings yet
- Constitutional Law Sem 5Document5 pagesConstitutional Law Sem 5Ichchhit SrivastavaNo ratings yet
- Audio Scripts B1 Student'S Book: CD 4 Track 38Document2 pagesAudio Scripts B1 Student'S Book: CD 4 Track 38Priscila De La Rosa0% (1)
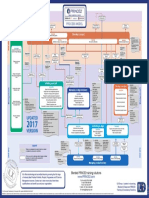
- p2 Process Model 2017Document1 pagep2 Process Model 2017Miguel Fernandes0% (1)
- Mécanisme de La Physionomie HumaineDocument2 pagesMécanisme de La Physionomie HumainebopufouriaNo ratings yet
- Constitution & By-LawsDocument15 pagesConstitution & By-LawsMichael C. AndradeNo ratings yet
- Labor Law Review Questions and AnswersDocument151 pagesLabor Law Review Questions and AnswersCarty MarianoNo ratings yet
- Section D Textual QuestionsDocument52 pagesSection D Textual Questionsxander ganderNo ratings yet
- Pdf-To-Word EditedDocument48 pagesPdf-To-Word EditedJames Genesis Ignacio LolaNo ratings yet
- MULTIPLE CHOICE. Choose The One Alternative That Best Completes The Statement or Answers The QuestionDocument6 pagesMULTIPLE CHOICE. Choose The One Alternative That Best Completes The Statement or Answers The QuestionBoshra BoshraNo ratings yet