You might also like
- Digital MedicineFrom EverandDigital MedicineArthur AndréNo ratings yet
- Principles Based Medical Informatics For Success NTDocument4 pagesPrinciples Based Medical Informatics For Success NTSvlader Reitef VanquisherNo ratings yet
- Information Technology Will Save Health Care: Institute of MedicineDocument7 pagesInformation Technology Will Save Health Care: Institute of MedicineKelvin Kurt B. AgwilangNo ratings yet
- TEMPEST: An Integrative Model For Health Technology AssessmentDocument15 pagesTEMPEST: An Integrative Model For Health Technology AssessmentRui AlmeidaNo ratings yet
- Tecnology 1Document7 pagesTecnology 1Anwaar JamalNo ratings yet
- ICT+in+healtcare OrangeDocument4 pagesICT+in+healtcare OrangeshubhamshklNo ratings yet
- Etelemed 2015 6 50 40284Document6 pagesEtelemed 2015 6 50 40284Martijn VeronNo ratings yet
- User Needs and Requirements Analysis For Big Data Healthcare ApplicationsDocument5 pagesUser Needs and Requirements Analysis For Big Data Healthcare Applicationsপ্রজ্ঞা লাবনীNo ratings yet
- Hgrid: An Economical Model For Mass-Health Care System Using Latest Technology (Grid Computing)Document5 pagesHgrid: An Economical Model For Mass-Health Care System Using Latest Technology (Grid Computing)IJMERNo ratings yet
- EPA02461 Acta Polytechnica 2019 02 163-181Document19 pagesEPA02461 Acta Polytechnica 2019 02 163-181liyun19981234No ratings yet
- ADAPT@AGENT - HOSPITAL: Agent-Based Optimization and Management of Clinical ProcessesDocument23 pagesADAPT@AGENT - HOSPITAL: Agent-Based Optimization and Management of Clinical Processeswalaba06No ratings yet
- Exercise 1Document2 pagesExercise 1TRISHA ISOBELLE ARBOLEDANo ratings yet
- Health Information Technology (HIT) Is "The Application of InformationDocument12 pagesHealth Information Technology (HIT) Is "The Application of InformationRahul GargNo ratings yet
- The Hospital Data Project: Comparing Hospital Activity Within EuropeDocument7 pagesThe Hospital Data Project: Comparing Hospital Activity Within EuropeDamian AlexandraNo ratings yet
- Proposal For An Implementation Framework For DigitDocument18 pagesProposal For An Implementation Framework For DigitAndréNo ratings yet
- ABSTRACT: The Emerging Proliferation of Fragmented: Temitayo - Fagbola@fuoye - Edu.ngDocument21 pagesABSTRACT: The Emerging Proliferation of Fragmented: Temitayo - Fagbola@fuoye - Edu.ngAnonymous jF8rU5No ratings yet
- Improving Sustainable Mobile Health Care Promotion - A Novel HybridDocument29 pagesImproving Sustainable Mobile Health Care Promotion - A Novel HybridojuNo ratings yet
- Moroccan Electronic Health Record System: Houssam BENBRAHIM, Hanaâ HACHIMI and Aouatif AMINEDocument8 pagesMoroccan Electronic Health Record System: Houssam BENBRAHIM, Hanaâ HACHIMI and Aouatif AMINESouhaïla MOUMOUNo ratings yet
- Artificial Intelligence in Medical Application: Electrical and Electronic Engineering DepartmentDocument18 pagesArtificial Intelligence in Medical Application: Electrical and Electronic Engineering Departmentمهيمن الابراهيميNo ratings yet
- Remote Health Monitoring of Elderly Through Wearable SensorsDocument26 pagesRemote Health Monitoring of Elderly Through Wearable SensorsAkansha SinghNo ratings yet
- 5 FuscoDocument10 pages5 FuscoZarah Alifani DzulhijjahNo ratings yet
- Doh2011 2013isspDocument191 pagesDoh2011 2013isspJay Pee CruzNo ratings yet
- Mhealth ReportDocument101 pagesMhealth ReportSteveEpsteinNo ratings yet
- E-Procurement in Hospital Pharmacies: An Exploratory Multi-Case Study From SwitzerlandDocument16 pagesE-Procurement in Hospital Pharmacies: An Exploratory Multi-Case Study From SwitzerlandPrudhvinadh KopparapuNo ratings yet
- HIS Implementation GuideDocument11 pagesHIS Implementation GuideJohn stevensonNo ratings yet
- P.kierkegaarde PrescriptionacrossEuropeDocument16 pagesP.kierkegaarde PrescriptionacrossEuropeseptiman zebuaNo ratings yet
- Digital HealthDocument5 pagesDigital HealthGloheal Test5No ratings yet
- E-Prescription Across Europe: Health and Technology September 2013Document16 pagesE-Prescription Across Europe: Health and Technology September 2013ifrahNo ratings yet
- Overview of ReportsDocument4 pagesOverview of ReportsMuhammad UmerNo ratings yet
- Role of ICT For HealthcareDocument13 pagesRole of ICT For HealthcareDejen AgaziuNo ratings yet
- 10 1 1 199Document10 pages10 1 1 199Pavel TudorNo ratings yet
- Covid + Digital TechDocument8 pagesCovid + Digital TechgraceNo ratings yet
- Implementation of EMRs, NigeriaDocument17 pagesImplementation of EMRs, NigeriaAsmamaw K.No ratings yet
- 1 PBDocument15 pages1 PBYat SonNo ratings yet
- Review Paper On Healthcare Monitoring SystemDocument9 pagesReview Paper On Healthcare Monitoring SystemEditor IJRITCCNo ratings yet
- HIMSS E-Health SIG White Paper: Access, Efficiency, Effectiveness, and Quality Improve The Health Status of PatientsDocument23 pagesHIMSS E-Health SIG White Paper: Access, Efficiency, Effectiveness, and Quality Improve The Health Status of PatientsSyed NasrullahNo ratings yet
- Design and Customization of Telemedicine SystemsDocument16 pagesDesign and Customization of Telemedicine SystemsNg Yi XuanNo ratings yet
- Research Article: Design and Customization of Telemedicine SystemsDocument17 pagesResearch Article: Design and Customization of Telemedicine SystemsBayu PrabuNo ratings yet
- Thesis Electronic Medical RecordsDocument6 pagesThesis Electronic Medical Recordscarmenmartinezmcallen100% (1)
- Official Lecture#4 - Overview of Health InformaticsDocument3 pagesOfficial Lecture#4 - Overview of Health InformaticsLYKA ANTONETTE ABREGANANo ratings yet
- DichDocument4 pagesDichngocphh.35No ratings yet
- Medicine of The Future Digital Technologies in HeaDocument10 pagesMedicine of The Future Digital Technologies in Heaeva kacanjaNo ratings yet
- Redp 4691Document34 pagesRedp 4691tonocovarruNo ratings yet
- Articulo en InglesDocument34 pagesArticulo en InglesJESUS GABRIEL VILLARREAL CUELLONo ratings yet
- Patient Information Systems in The LiteratureDocument6 pagesPatient Information Systems in The LiteratureJohn MunaonyediNo ratings yet
- AmirLatif2020 Article ARemixIDESmartContract-basedFrDocument24 pagesAmirLatif2020 Article ARemixIDESmartContract-basedFrDivya KandpalNo ratings yet
- Discussion Paper On Semantic and Technical InteroperabilityDocument7 pagesDiscussion Paper On Semantic and Technical InteroperabilityΜΙΚΕNo ratings yet
- Role of ICT in HealthcareDocument19 pagesRole of ICT in HealthcareRama VenugopalNo ratings yet
- Ecommerce's Important Role in The Medical Sector: Luzanna Fung Lok Chee and Rashad YazdanifardDocument8 pagesEcommerce's Important Role in The Medical Sector: Luzanna Fung Lok Chee and Rashad YazdanifardAsora Yasmin snehaNo ratings yet
- LIMBAH MEDIS klmpk5Document9 pagesLIMBAH MEDIS klmpk5Hesti FinoNo ratings yet
- Software Engineering in HealthcareDocument5 pagesSoftware Engineering in HealthcareIJRASETPublicationsNo ratings yet
- Implementing Telemedicine in Afghanistan-Challenges and Issue1Document6 pagesImplementing Telemedicine in Afghanistan-Challenges and Issue1Muhibullah AmanNo ratings yet
- Potsdam ConferenceDocument21 pagesPotsdam ConferenceheeducationalservicesNo ratings yet
- Project ProposalDocument9 pagesProject ProposalMike Mwesh BernardNo ratings yet
- It in Health CareDocument8 pagesIt in Health CareAnnonymous963258No ratings yet
- Cybersecurity Match Supply and Demand in Portuguese HealthCare Sector Industry Collaboration - Reviewed FinalDocument13 pagesCybersecurity Match Supply and Demand in Portuguese HealthCare Sector Industry Collaboration - Reviewed FinalRui GomesNo ratings yet
- Bluemine - Applying Analytics in HealthcareDocument16 pagesBluemine - Applying Analytics in HealthcareRaam MkNo ratings yet
- TelemedicineDocument6 pagesTelemedicineMarcNo ratings yet
- Proposed System Using Iot and Gis To Generate Electronic Medical RecordsDocument11 pagesProposed System Using Iot and Gis To Generate Electronic Medical Recordsindex PubNo ratings yet
- Suspension Block AssemblyDocument1 pageSuspension Block AssemblymamatnamakuNo ratings yet
- Derailleur Chain Tensioner Idlers Etc.: Fig CT4Document1 pageDerailleur Chain Tensioner Idlers Etc.: Fig CT4mamatnamakuNo ratings yet
- Toolkit Included in The Toolkit: DATA SHEET: Ds-Toolkit ISSUE S1001Document2 pagesToolkit Included in The Toolkit: DATA SHEET: Ds-Toolkit ISSUE S1001mamatnamakuNo ratings yet
- Retro-Fitting L-Type Mudguards:: Aug-10 Mglret DsDocument4 pagesRetro-Fitting L-Type Mudguards:: Aug-10 Mglret DsmamatnamakuNo ratings yet
- Wheels Rims and Spokes Important Information: DATA SHEET: Ds-Wheel ISSUE S1004Document1 pageWheels Rims and Spokes Important Information: DATA SHEET: Ds-Wheel ISSUE S1004mamatnamakuNo ratings yet
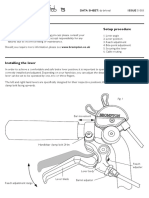
- Brake Lever Setup Important Information Setup Procedure: DATA SHEET: Ds-Brleval ISSUE S1003Document2 pagesBrake Lever Setup Important Information Setup Procedure: DATA SHEET: Ds-Brleval ISSUE S1003mamatnamakuNo ratings yet
- This Luggage Item Is NOT Suitable For Use With A Brompton S-Type ModelDocument2 pagesThis Luggage Item Is NOT Suitable For Use With A Brompton S-Type ModelmamatnamakuNo ratings yet
- These Notes Relate Mainly To Fitting A New Pillar, But They May Also Be Helpful When Exchanging Certain PartsDocument2 pagesThese Notes Relate Mainly To Fitting A New Pillar, But They May Also Be Helpful When Exchanging Certain PartsmamatnamakuNo ratings yet
- Fig GTR1: Aug-10 Gtrigb3 DsDocument3 pagesFig GTR1: Aug-10 Gtrigb3 DsmamatnamakuNo ratings yet
- Lamp Brackets / Battery Lights.: Jan-12 Batlam DsDocument4 pagesLamp Brackets / Battery Lights.: Jan-12 Batlam DsmamatnamakuNo ratings yet
- DJI Spark DesignDocument1 pageDJI Spark DesignmamatnamakuNo ratings yet
- Fibrous JointDocument5 pagesFibrous JointmamatnamakuNo ratings yet
- Derailleur Chain Tensioner Idlers Etc.: Fig CT4Document1 pageDerailleur Chain Tensioner Idlers Etc.: Fig CT4mamatnamakuNo ratings yet
- BS en 14885-2015Document64 pagesBS en 14885-2015mamatnamaku100% (3)
- Xtrail t32Document113 pagesXtrail t32mamatnamakuNo ratings yet
- BS en 16615-2015Document44 pagesBS en 16615-2015mamatnamaku100% (7)
- BS en 16616-2015Document40 pagesBS en 16616-2015mamatnamaku100% (3)
- INTR - Indonesia National Trade Repository PDFDocument4 pagesINTR - Indonesia National Trade Repository PDFmamatnamakuNo ratings yet
- Computer Science: From Wikipedia, The Free EncyclopediaDocument15 pagesComputer Science: From Wikipedia, The Free EncyclopediamamatnamakuNo ratings yet
- Validation EtoDocument8 pagesValidation EtomamatnamakuNo ratings yet
- Virtualization: Old Technology Offers Huge New Potential: Greg GothDocument4 pagesVirtualization: Old Technology Offers Huge New Potential: Greg GothmamatnamakuNo ratings yet
- 1-A Business Model Framework For The Design and Evaluation of Business Models in The Internet of ServicesDocument13 pages1-A Business Model Framework For The Design and Evaluation of Business Models in The Internet of ServicesmamatnamakuNo ratings yet
- Downey L, Lloyd H - Bed Bathing Patients in Hospital - ArticleDocument6 pagesDowney L, Lloyd H - Bed Bathing Patients in Hospital - Articlemamatnamaku100% (1)
- M750 Service ManualDocument78 pagesM750 Service ManualcciprainNo ratings yet
- Oracle HCM Cloud OverviewDocument35 pagesOracle HCM Cloud OverviewAngelVillalobosNo ratings yet
- Element Description Team CharterDocument2 pagesElement Description Team CharterPRASHANT GUPTANo ratings yet
- CMPE 011 Reviewer MidtermsDocument5 pagesCMPE 011 Reviewer MidtermsJohn Rave Manuel GonzalesNo ratings yet
- Module 2 - Physical Presentation of Reports LettersDocument14 pagesModule 2 - Physical Presentation of Reports Lettersashutoshsk5120% (1)
- SMI983Document8 pagesSMI983ade.achielNo ratings yet
- Sunlight StyleGuide DataViz PDFDocument13 pagesSunlight StyleGuide DataViz PDFSai Kiran AdepuNo ratings yet
- Lecture1Document51 pagesLecture1Kimberley Oh100% (1)
- Jual Sokkia SET 350X Total Station - Harga, Spesifikasi Dan ReviewDocument5 pagesJual Sokkia SET 350X Total Station - Harga, Spesifikasi Dan Reviewbramsalwa2676No ratings yet
- Samsung Group: By: Ethel Herna C. PabitoDocument13 pagesSamsung Group: By: Ethel Herna C. PabitoEthel PabitoNo ratings yet
- Buku Standarisasi Spek Mtu PLN - SK Dir 216 (Bus VT)Document1 pageBuku Standarisasi Spek Mtu PLN - SK Dir 216 (Bus VT)PontasNo ratings yet
- Energy Modeling GuidelinesDocument32 pagesEnergy Modeling GuidelinesBrian MayNo ratings yet
- Deep Learning For Audio Signal ProcessingDocument14 pagesDeep Learning For Audio Signal Processingsantoshmore439No ratings yet
- HP Mouse TestDocument8 pagesHP Mouse Testradiophon666No ratings yet
- EpayDocument17 pagesEpayShrinivas PrabhuneNo ratings yet
- Guide: Performance Optimization For The Galileo 10 Runtime SystemDocument15 pagesGuide: Performance Optimization For The Galileo 10 Runtime Systemvaldemir huculakNo ratings yet
- Evault MAX 80128223 UL 9540A Test ReportDocument38 pagesEvault MAX 80128223 UL 9540A Test Reportjaikp56No ratings yet
- Solar SystemsDocument23 pagesSolar SystemsRaghavendra RaghavNo ratings yet
- BS 6349-2Document64 pagesBS 6349-2medianna100% (6)
- NEXYGENPlus Spec SheetDocument3 pagesNEXYGENPlus Spec Sheetrossifam777No ratings yet
- Forza XADV 750 - 2021 Program SmartkeyDocument8 pagesForza XADV 750 - 2021 Program SmartkeyAny TimNo ratings yet
- Brochure Liebert ITA Series (5-20KVA)Document4 pagesBrochure Liebert ITA Series (5-20KVA)kimxoNo ratings yet
- Migrate MySQL Database To Azure Database For Mysql OnlineDocument11 pagesMigrate MySQL Database To Azure Database For Mysql Onlinethecoinmaniac hodlNo ratings yet
- Lab Report No 10ADCDocument4 pagesLab Report No 10ADCIhsan ul HaqNo ratings yet
- Machine Learning Lab Manual 8Document12 pagesMachine Learning Lab Manual 8Raheel AslamNo ratings yet
- Non Volatile MemoryDocument16 pagesNon Volatile MemoryvinutkumarNo ratings yet
- 190-01499-00 - F - Pilot GuideDocument34 pages190-01499-00 - F - Pilot GuideFordiNo ratings yet
- Section 1 - Paperi-General Knowledge and Current Affairs: Set Id: 53449 - 6Document19 pagesSection 1 - Paperi-General Knowledge and Current Affairs: Set Id: 53449 - 6babluNo ratings yet
- Mihai Nicusor: Curriculum Vitae Replace With First Name(s) Surname(s)Document2 pagesMihai Nicusor: Curriculum Vitae Replace With First Name(s) Surname(s)Nicusor MihaiNo ratings yet
- 3bhs212794 E01 Revn User Manual Acs6000Document266 pages3bhs212794 E01 Revn User Manual Acs6000Fernando RamirezNo ratings yet