You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Brain Circuitry and Signaling in PsychiatryDocument281 pagesBrain Circuitry and Signaling in Psychiatryruca_m_noronha75% (4)
- BC 07 2004 The Functional Neuroanatomy of AggressionDocument29 pagesBC 07 2004 The Functional Neuroanatomy of Aggressionmacplenty100% (5)
- Progress in NeurobiologyDocument14 pagesProgress in NeurobiologyAqua ToffanaNo ratings yet
- Monument of Myth: The Basilica of Sacre CouerDocument20 pagesMonument of Myth: The Basilica of Sacre CouerGeneric_PersonaNo ratings yet
- Agenda Setting, Public Opinion & Immigration ReformDocument21 pagesAgenda Setting, Public Opinion & Immigration ReformGeneric_PersonaNo ratings yet
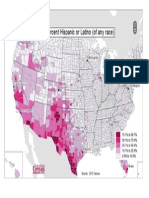
- US Map of Hispanic Population by CountyDocument1 pageUS Map of Hispanic Population by CountyGeneric_PersonaNo ratings yet
- Crown & Baptist Streets Village Group: ST Re EtDocument1 pageCrown & Baptist Streets Village Group: ST Re EtGeneric_PersonaNo ratings yet
- The Diversity of Debt Crises in EuropeDocument18 pagesThe Diversity of Debt Crises in EuropeGeneric_PersonaNo ratings yet
- Sydney Australia's Green Sector OpportunityDocument8 pagesSydney Australia's Green Sector OpportunityGeneric_PersonaNo ratings yet
- Earnings of ImmigrantsDocument23 pagesEarnings of ImmigrantsGeneric_PersonaNo ratings yet
- The Rise of The Individual in Modern ChinaDocument3 pagesThe Rise of The Individual in Modern ChinaGeneric_PersonaNo ratings yet
- Result of Portrayals of Latinos On TVDocument33 pagesResult of Portrayals of Latinos On TVGeneric_PersonaNo ratings yet
- Sydney As A Global CityDocument9 pagesSydney As A Global CityGeneric_PersonaNo ratings yet
- Peach Leaf CurlDocument3 pagesPeach Leaf CurlGeneric_PersonaNo ratings yet
- Risk-Managing Revolution (Arab Spring)Document4 pagesRisk-Managing Revolution (Arab Spring)Generic_PersonaNo ratings yet
- Citizens United ReviewDocument5 pagesCitizens United ReviewGeneric_PersonaNo ratings yet
- China and Sydney Australias Growing Business PartnershipDocument8 pagesChina and Sydney Australias Growing Business PartnershipGeneric_PersonaNo ratings yet
- English Language in Hong KongDocument13 pagesEnglish Language in Hong KongGeneric_PersonaNo ratings yet
- Measuring Helix Angle of GearsDocument6 pagesMeasuring Helix Angle of Gearsdarshan.hegdebNo ratings yet
- Empowering Youth - Technology in Advocacy To Affect Social ChangeDocument18 pagesEmpowering Youth - Technology in Advocacy To Affect Social ChangeGeneric_PersonaNo ratings yet
- Grizzly Hevy Duty Wood Lathe ManualDocument60 pagesGrizzly Hevy Duty Wood Lathe ManualGeneric_PersonaNo ratings yet
- Protests in An Information SocietyDocument25 pagesProtests in An Information SocietyGeneric_PersonaNo ratings yet
- US Policy and The International Dimensions of Failed Democratic Transitions in The Arab WorldDocument18 pagesUS Policy and The International Dimensions of Failed Democratic Transitions in The Arab WorldGeneric_PersonaNo ratings yet
- Educated Preferences: Explaining Attitudes Toward Immigration in EuropeDocument44 pagesEducated Preferences: Explaining Attitudes Toward Immigration in EuropeGeneric_PersonaNo ratings yet
- Promoting Economic Liberalization in EgyptDocument14 pagesPromoting Economic Liberalization in EgyptGeneric_PersonaNo ratings yet
- English Language in Hong KongDocument13 pagesEnglish Language in Hong KongGeneric_PersonaNo ratings yet
- A Study On The Effects of Sexually Explicit Advertisement On MemoryDocument10 pagesA Study On The Effects of Sexually Explicit Advertisement On MemoryGeneric_PersonaNo ratings yet
- The Rise of The Individual in Modern ChinaDocument3 pagesThe Rise of The Individual in Modern ChinaGeneric_PersonaNo ratings yet
- Internet, Mass Communication & Collective ActionDocument12 pagesInternet, Mass Communication & Collective ActionGeneric_PersonaNo ratings yet
- Prilleltensky.2008.Role of Power in Wellness-Oppression-Liberation - JCP PDFDocument21 pagesPrilleltensky.2008.Role of Power in Wellness-Oppression-Liberation - JCP PDFcastrolaNo ratings yet
- Title Insert (Derogatory Words) Research StudyDocument5 pagesTitle Insert (Derogatory Words) Research StudyGeneric_PersonaNo ratings yet
- Hypothalamic Astrocytoma: Hyperphagia Syndrome & Accompanying IssuesDocument4 pagesHypothalamic Astrocytoma: Hyperphagia Syndrome & Accompanying IssuesGeneric_PersonaNo ratings yet
- Brand Effect in CoffeeDocument4 pagesBrand Effect in CoffeeDhiraj AgrawalNo ratings yet
- University of SkovdaDocument44 pagesUniversity of SkovdaKetaki RautNo ratings yet
- Brain Circuit Dysfunction in Post - Traumatic Stress Disorder: From Mouse To Man - Robert J. FensterDocument17 pagesBrain Circuit Dysfunction in Post - Traumatic Stress Disorder: From Mouse To Man - Robert J. FensterAlvaro Arboledas LoriteNo ratings yet
- Brune 2006Document14 pagesBrune 2006Dr. Kaushal Kishor SharmaNo ratings yet
- The Adolescent Brain - Casey 2008Document26 pagesThe Adolescent Brain - Casey 2008Ramona AnisieNo ratings yet
- Cognitive Impairment. Causes, Diagnosis and Treatment PDFDocument257 pagesCognitive Impairment. Causes, Diagnosis and Treatment PDFCris RaNo ratings yet
- Contributions of The InsulaDocument11 pagesContributions of The Insulaninaesba-1No ratings yet
- Task-Dependent Neural Correlates of The Processing of Verbal Threat-Related Stimuli in Social PhobiaDocument9 pagesTask-Dependent Neural Correlates of The Processing of Verbal Threat-Related Stimuli in Social PhobiaTony StarkNo ratings yet
- Traumatic Stress: Effects On The BrainDocument17 pagesTraumatic Stress: Effects On The BrainAnonymous 9NMg0Be5WTNo ratings yet
- Music Therapy PDFDocument8 pagesMusic Therapy PDFRamo123No ratings yet
- Anxiety and Affective Style: Role of Prefrontal Cortex and AmygdalaDocument13 pagesAnxiety and Affective Style: Role of Prefrontal Cortex and AmygdalaSamir Castolo SanchezNo ratings yet
- Introduction to Behavioral Addictions: Comparing Impulse Control Disorders and Substance UseDocument15 pagesIntroduction to Behavioral Addictions: Comparing Impulse Control Disorders and Substance UsenishthasainiNo ratings yet
- Jurnal 3Document19 pagesJurnal 3Belajar KedokteranNo ratings yet
- Mindfulness Training and Neural Integration: Differentiation of Distinct Streams of Awareness and The Cultivation of Well-BeingDocument5 pagesMindfulness Training and Neural Integration: Differentiation of Distinct Streams of Awareness and The Cultivation of Well-BeingGretchen Marie Aristud AquinoNo ratings yet
- Affective Neuroscience and PsychopathologyDocument78 pagesAffective Neuroscience and PsychopathologyLucíaNo ratings yet
- Neurochemistry of MusicDocument15 pagesNeurochemistry of MusicLisa CerezoNo ratings yet
- Neuropsychology of Anxiety DisordersDocument29 pagesNeuropsychology of Anxiety DisordersnivethaNo ratings yet
- Fuster 2001Document15 pagesFuster 2001Jane SmithNo ratings yet
- The Psychopath MagnetizedDocument9 pagesThe Psychopath MagnetizedAvengingBrainNo ratings yet
- Fred TravisDocument8 pagesFred TravisMeditatia Transcendentala Romania100% (1)
- The Neuroscience of Depressive Disorders - A Brief Review of The Past and Some Considerations About The FutureDocument6 pagesThe Neuroscience of Depressive Disorders - A Brief Review of The Past and Some Considerations About The FutureRaúl VerdugoNo ratings yet
- Bachevalier2006 Orbitofrontal-ADocument21 pagesBachevalier2006 Orbitofrontal-AOni BlenginoNo ratings yet
- Circuitos de La AdiccionDocument28 pagesCircuitos de La AdiccionJose Andres AlvarezNo ratings yet
- A Step Towards Personalized Sports Nutrition PDFDocument9 pagesA Step Towards Personalized Sports Nutrition PDFJMedeirosNo ratings yet
- A Neurobiological Model of Borderline PersonalityDocument19 pagesA Neurobiological Model of Borderline Personalityme13No ratings yet
- Speech ModelDocument10 pagesSpeech ModelRafael AlvesNo ratings yet
- Adolphs R.-Cognitive Neuroscience of Human Social Behaviour (2003) PDFDocument14 pagesAdolphs R.-Cognitive Neuroscience of Human Social Behaviour (2003) PDFngonzalezduran5920100% (1)