You might also like
- Article The Nurse S Role in Helping Older People To Use The ToiletDocument5 pagesArticle The Nurse S Role in Helping Older People To Use The ToiletAnonymous hnk5L17No ratings yet
- Lec NCM 100Document27 pagesLec NCM 100Jay DavidNo ratings yet
- Lydia HallDocument2 pagesLydia HallHazel ZullaNo ratings yet
- The Complete Guide to Nursing and Interview Questions and AnswersFrom EverandThe Complete Guide to Nursing and Interview Questions and AnswersNo ratings yet
- Fundamentals of Nursing Week12 2Document49 pagesFundamentals of Nursing Week12 2alyssatorillo22No ratings yet
- Humanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperFrom EverandHumanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperNo ratings yet
- Personal Hygiene: Mary Grace L. Araullo RN MSCPDDocument23 pagesPersonal Hygiene: Mary Grace L. Araullo RN MSCPDgraceNo ratings yet
- Nurs04 WK4Document10 pagesNurs04 WK4MARY ROSE FAJUTINANo ratings yet
- Incontinence CareDocument7 pagesIncontinence Careapi-308965846No ratings yet
- Midwife-Led Units, Community Midwifery Units and Birth CentresDocument13 pagesMidwife-Led Units, Community Midwifery Units and Birth CentresLara AldazNo ratings yet
- FOSTERING DIGNITY AND RESPECT IN CARE NewDocument5 pagesFOSTERING DIGNITY AND RESPECT IN CARE NewSidra Waqar KhanNo ratings yet
- FOSTERING DIGNITY AND RESPECT IN CARE NewDocument5 pagesFOSTERING DIGNITY AND RESPECT IN CARE NewSidra Waqar Khan100% (2)
- Nursing As A Profession: by Jeelani SaimaDocument53 pagesNursing As A Profession: by Jeelani Saimajeelani saimaNo ratings yet
- 0010 - ETHOS OF NURSING PRACTICE Full Note PDFDocument48 pages0010 - ETHOS OF NURSING PRACTICE Full Note PDFRicardo Domingos100% (1)
- Research TitleDocument4 pagesResearch TitlebnellaNo ratings yet
- Principles and Fundamentals of NursingDocument1,060 pagesPrinciples and Fundamentals of Nursingkariuki90406978No ratings yet
- C304 Task 1 Word A PDFDocument33 pagesC304 Task 1 Word A PDFCamille Joy BaliliNo ratings yet
- Nurses' Roles and Responsibilities in Providing Care and Support at The End of LifeDocument10 pagesNurses' Roles and Responsibilities in Providing Care and Support at The End of Lifededsec hackerNo ratings yet
- Perioperative NursingDocument103 pagesPerioperative NursingRochelle Anne SorioNo ratings yet
- Introduction To NDocument42 pagesIntroduction To NS. KNo ratings yet
- Gibbs Reflective Journal SampleDocument4 pagesGibbs Reflective Journal SampleCres Padua Quinzon100% (2)
- Clinical Methods: Nursing RoundsDocument7 pagesClinical Methods: Nursing RoundsYAMINIPRIYANNo ratings yet
- LeiningerDocument36 pagesLeiningerAshley EmperadorNo ratings yet
- Presentation Transcultural NursingDocument23 pagesPresentation Transcultural NursingHazel Eñga Tiam Wat100% (2)
- AdvocacyinnursingDocument5 pagesAdvocacyinnursingjkm36403No ratings yet
- Futuristic NursingDocument14 pagesFuturistic NursingHarpreet Dhatt50% (4)
- Chapter 1-3Document26 pagesChapter 1-3Jemimah Ruth Madayag Valenzuela100% (1)
- #175670601Document5 pages#175670601freelance writerNo ratings yet
- Fundamentals of Professional NursingDocument50 pagesFundamentals of Professional NursingKwasi PatrickNo ratings yet
- Autonomy, HospitalityDocument12 pagesAutonomy, HospitalityDr. Mohammed SayedNo ratings yet
- Log 3 NIP1003: C Bogateanu M00526321Document6 pagesLog 3 NIP1003: C Bogateanu M00526321trandafirashNo ratings yet
- Nursing ServiceDocument97 pagesNursing ServicePragyashaa ChaudharyNo ratings yet
- Fundamentals of Nursing - 1Document1,794 pagesFundamentals of Nursing - 1Emmanuel Kiprono100% (1)
- Code of Ethics: RightsDocument15 pagesCode of Ethics: Rightsmarilen099No ratings yet
- Nursing Ethnography Final DraftDocument9 pagesNursing Ethnography Final Draftapi-315823367No ratings yet
- 9780199237838Document11 pages9780199237838Jasmine Ann Catherine Price100% (1)
- Florence Nightingale (Environmental Theory)Document23 pagesFlorence Nightingale (Environmental Theory)Irah A.No ratings yet
- Faye Glenn Abdellah S Nursing TheoryDocument11 pagesFaye Glenn Abdellah S Nursing TheoryJeffrey Ian M. KoNo ratings yet
- 2022 Nurses Week PresentationDocument19 pages2022 Nurses Week PresentationMargaret DigitemieNo ratings yet
- The Role of The Charge Nurse: What I Believe It To Be, Why I Am Here and What I Could Offer To The RoleDocument25 pagesThe Role of The Charge Nurse: What I Believe It To Be, Why I Am Here and What I Could Offer To The RoleAlan George BevanNo ratings yet
- Nursing TheoriesDocument3 pagesNursing TheoriesAyessa Camelle DumileNo ratings yet
- Leininger2 - Culture Care Universality & DiversityDocument32 pagesLeininger2 - Culture Care Universality & Diversitymao ayunan (misaki minna ayunan)No ratings yet
- TransculturalDocument13 pagesTransculturalDONALDNo ratings yet
- Patient Autonomy A View From The KitchenDocument10 pagesPatient Autonomy A View From The KitchenTin Ker JoNo ratings yet
- Nursing TheoristsDocument97 pagesNursing TheoristsMarti GregorioNo ratings yet
- Example Literature Review Hand WashingDocument7 pagesExample Literature Review Hand Washingmtxziixgf100% (1)
- Program ProposalDocument14 pagesProgram ProposalJoey Dee Bravo100% (1)
- Faye Glenn AbdellahDocument12 pagesFaye Glenn AbdellahAnnapurna Dangeti100% (1)
- Assessment 2 Cultural SafetyDocument2 pagesAssessment 2 Cultural SafetyMahal PaetNo ratings yet
- Nursing FoundationDocument200 pagesNursing FoundationManu CvNo ratings yet
- Mortensene ApasafetyqualityDocument5 pagesMortensene Apasafetyqualityapi-284786443No ratings yet
- cs4 Case StudyDocument7 pagescs4 Case Studyapi-436279390No ratings yet
- Nursing Autonomy and Responsibilities To Family MembersDocument4 pagesNursing Autonomy and Responsibilities To Family MembersKoEy Are UNo ratings yet
- Nursng ReportDocument19 pagesNursng ReportNgurahNo ratings yet
- Nursing TheoriesDocument7 pagesNursing TheoriesemsdaxxNo ratings yet
- A Case Study From A Cultural PerspectiveDocument4 pagesA Case Study From A Cultural Perspectiveapi-436279390No ratings yet
- Trancultural Nursing: EssayDocument6 pagesTrancultural Nursing: EssayJoko Tri WahyudiNo ratings yet
- Retro-Fitting L-Type Mudguards:: Aug-10 Mglret DsDocument4 pagesRetro-Fitting L-Type Mudguards:: Aug-10 Mglret DsmamatnamakuNo ratings yet
- Toolkit Included in The Toolkit: DATA SHEET: Ds-Toolkit ISSUE S1001Document2 pagesToolkit Included in The Toolkit: DATA SHEET: Ds-Toolkit ISSUE S1001mamatnamakuNo ratings yet
- Suspension Block AssemblyDocument1 pageSuspension Block AssemblymamatnamakuNo ratings yet
- Wheels Rims and Spokes Important Information: DATA SHEET: Ds-Wheel ISSUE S1004Document1 pageWheels Rims and Spokes Important Information: DATA SHEET: Ds-Wheel ISSUE S1004mamatnamakuNo ratings yet
- Fig GTR1: Aug-10 Gtrigb3 DsDocument3 pagesFig GTR1: Aug-10 Gtrigb3 DsmamatnamakuNo ratings yet
- Derailleur Chain Tensioner Idlers Etc.: Fig CT4Document1 pageDerailleur Chain Tensioner Idlers Etc.: Fig CT4mamatnamakuNo ratings yet
- These Notes Relate Mainly To Fitting A New Pillar, But They May Also Be Helpful When Exchanging Certain PartsDocument2 pagesThese Notes Relate Mainly To Fitting A New Pillar, But They May Also Be Helpful When Exchanging Certain PartsmamatnamakuNo ratings yet
- BS en 14885-2015Document64 pagesBS en 14885-2015mamatnamaku100% (3)
- INTR - Indonesia National Trade Repository PDFDocument4 pagesINTR - Indonesia National Trade Repository PDFmamatnamakuNo ratings yet
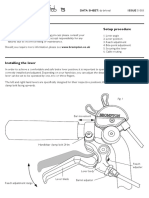
- Brake Lever Setup Important Information Setup Procedure: DATA SHEET: Ds-Brleval ISSUE S1003Document2 pagesBrake Lever Setup Important Information Setup Procedure: DATA SHEET: Ds-Brleval ISSUE S1003mamatnamakuNo ratings yet
- Lamp Brackets / Battery Lights.: Jan-12 Batlam DsDocument4 pagesLamp Brackets / Battery Lights.: Jan-12 Batlam DsmamatnamakuNo ratings yet
- Derailleur Chain Tensioner Idlers Etc.: Fig CT4Document1 pageDerailleur Chain Tensioner Idlers Etc.: Fig CT4mamatnamakuNo ratings yet
- This Luggage Item Is NOT Suitable For Use With A Brompton S-Type ModelDocument2 pagesThis Luggage Item Is NOT Suitable For Use With A Brompton S-Type ModelmamatnamakuNo ratings yet
- CHAIN TENSIONER DISC Cta - DsDocument4 pagesCHAIN TENSIONER DISC Cta - DsAgus SujantoNo ratings yet
- Derailleur Chain Tensioner Idlers Etc.: Fig CT4Document1 pageDerailleur Chain Tensioner Idlers Etc.: Fig CT4mamatnamakuNo ratings yet
- BS en 16615-2015Document44 pagesBS en 16615-2015mamatnamaku100% (7)
- BS en 16616-2015Document40 pagesBS en 16616-2015mamatnamaku100% (3)
- Fibrous JointDocument5 pagesFibrous JointmamatnamakuNo ratings yet
- BS en 01040-2005Document44 pagesBS en 01040-2005mamatnamaku100% (5)
- Validation EtoDocument8 pagesValidation EtomamatnamakuNo ratings yet
- Xtrail t32Document113 pagesXtrail t32mamatnamakuNo ratings yet
- BS en 01040-2005Document44 pagesBS en 01040-2005mamatnamaku100% (5)
- DJI Spark DesignDocument1 pageDJI Spark DesignmamatnamakuNo ratings yet
- E ShoppingDocument11 pagesE ShoppingZil ShahNo ratings yet
- Virtualization: Old Technology Offers Huge New Potential: Greg GothDocument4 pagesVirtualization: Old Technology Offers Huge New Potential: Greg GothmamatnamakuNo ratings yet
- Cdc-Guideline For Disinfection and Sterilization in Health-Care Facilities-2008Document158 pagesCdc-Guideline For Disinfection and Sterilization in Health-Care Facilities-2008fuentenatura100% (1)
- Class II Special Controls Guidance Document Surgical SuturesDocument12 pagesClass II Special Controls Guidance Document Surgical Sutures601026No ratings yet
- Computer Science: From Wikipedia, The Free EncyclopediaDocument15 pagesComputer Science: From Wikipedia, The Free EncyclopediamamatnamakuNo ratings yet
- Pembagian Kelas Alat Kesehatan Perkategori ProdukDocument41 pagesPembagian Kelas Alat Kesehatan Perkategori Produkdimitrijm100% (1)
- 1-A Business Model Framework For The Design and Evaluation of Business Models in The Internet of ServicesDocument13 pages1-A Business Model Framework For The Design and Evaluation of Business Models in The Internet of ServicesmamatnamakuNo ratings yet
- Proc PDF FileDocument8 pagesProc PDF FileVivek GutamNo ratings yet
- Management of Patients With Hepatocellular Carcinoma (HCC) : H P B (HPB) F C GDocument15 pagesManagement of Patients With Hepatocellular Carcinoma (HCC) : H P B (HPB) F C GFloyd balansagNo ratings yet
- UPSIDC Bylaws 17052017 PDFDocument193 pagesUPSIDC Bylaws 17052017 PDFPraveen kumarNo ratings yet
- Eaglet Volume 56 # 3 SY 2009-2010Document40 pagesEaglet Volume 56 # 3 SY 2009-2010Mara Melanie D. PerezNo ratings yet
- Medical Tourism in IndiaDocument23 pagesMedical Tourism in IndiaIndu ShekharNo ratings yet
- Annual Report 2008Document32 pagesAnnual Report 2008vnatcNo ratings yet
- Lhay Project UnfinishedDocument26 pagesLhay Project UnfinishedLhay WafuNo ratings yet
- Lone Star Shopper: Johnnie StoneDocument12 pagesLone Star Shopper: Johnnie StoneCoolerAdsNo ratings yet
- Nowell Ona CVDocument3 pagesNowell Ona CVNowell Ona AdmsNo ratings yet
- Kibera Mirror MayDocument8 pagesKibera Mirror Mayvincent achuka maisibaNo ratings yet
- Starting A PharmacyDocument8 pagesStarting A PharmacyLloyd Fyl O. RazoNo ratings yet
- FIP PharmabridgeDocument2 pagesFIP PharmabridgeInternational Pharmaceutical Students' Federation (IPSF)No ratings yet
- DM PH&SD P4 TG17 (Guidelines+for+First Aid+Requirement)Document0 pagesDM PH&SD P4 TG17 (Guidelines+for+First Aid+Requirement)ahmedspecbvNo ratings yet
- Posttest. Renal DisordersDocument3 pagesPosttest. Renal Disordersjbagacay100% (3)
- Some RRLDocument3 pagesSome RRLOmar Christian TuazonNo ratings yet
- TDocument5 pagesTShwardz PamittanNo ratings yet
- SPF's Love and Peace MagazineDocument80 pagesSPF's Love and Peace MagazinekishwarNo ratings yet
- 1Document94 pages1Emanuel Acray Nkondola100% (2)
- 27th SFTC Biam BograDocument5 pages27th SFTC Biam BograPritam RoyNo ratings yet
- Case Study:: Maitreya-Buddha PyramidDocument3 pagesCase Study:: Maitreya-Buddha PyramidShreenivasan Muthukumarasamy100% (6)
- 2017 UB04 Hospital Instructions-Final 8FEB2018Document99 pages2017 UB04 Hospital Instructions-Final 8FEB2018krishna EnagaluruNo ratings yet
- A Study On Effectiveness of Promotional Strategy of AMRI Hospital DhakuriaDocument53 pagesA Study On Effectiveness of Promotional Strategy of AMRI Hospital DhakuriaGourab Majumder50% (2)
- Organogram HospitalDocument1 pageOrganogram HospitalNisha BhimsariaNo ratings yet
- Healing Gardens FinalDocument20 pagesHealing Gardens FinalMohd Salahuddin100% (1)
- Professor HieronimusDocument341 pagesProfessor Hieronimusbob robNo ratings yet
- To Whom It May ConcernDocument8 pagesTo Whom It May ConcernKaren EstavilloNo ratings yet
- Thyroidectomy NCPDocument3 pagesThyroidectomy NCPKim Enrico Jumarang100% (2)
- INVESTMENT MEMO - TanzaniteDocument5 pagesINVESTMENT MEMO - TanzaniteSuresh PoojariNo ratings yet
- London'S Top 50 Wellbeing Gurus: Thelondonnews ThelondonnewsDocument1 pageLondon'S Top 50 Wellbeing Gurus: Thelondonnews ThelondonnewsAlireza HemmatiNo ratings yet
- Patient Safety and Patient Assessment in Pre-Hospital Care: A Study ProtocolDocument7 pagesPatient Safety and Patient Assessment in Pre-Hospital Care: A Study ProtocolDeby KurniawanNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1459)
- Briefly Perfectly Human: Making an Authentic Life by Getting Real About the EndFrom EverandBriefly Perfectly Human: Making an Authentic Life by Getting Real About the EndNo ratings yet
- No Mud, No Lotus: The Art of Transforming SufferingFrom EverandNo Mud, No Lotus: The Art of Transforming SufferingRating: 5 out of 5 stars5/5 (175)
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerFrom EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerRating: 4.5 out of 5 stars4.5/5 (58)
- Prisoners of Geography: Ten Maps That Explain Everything About the WorldFrom EverandPrisoners of Geography: Ten Maps That Explain Everything About the WorldRating: 4.5 out of 5 stars4.5/5 (1145)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipFrom EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipRating: 4.5 out of 5 stars4.5/5 (1135)
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissFrom EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissRating: 4.5 out of 5 stars4.5/5 (82)
- Peaceful Sleep Hypnosis: Meditate & RelaxFrom EverandPeaceful Sleep Hypnosis: Meditate & RelaxRating: 4.5 out of 5 stars4.5/5 (142)
- The Bridesmaid: The addictive psychological thriller that everyone is talking aboutFrom EverandThe Bridesmaid: The addictive psychological thriller that everyone is talking aboutRating: 4 out of 5 stars4/5 (131)
- Neville Goddard Master Course to Manifest Your Desires Into Reality Using The Law of Attraction: Learn the Secret to Overcoming Your Current Problems and Limitations, Attaining Your Goals, and Achieving Health, Wealth, Happiness and Success!From EverandNeville Goddard Master Course to Manifest Your Desires Into Reality Using The Law of Attraction: Learn the Secret to Overcoming Your Current Problems and Limitations, Attaining Your Goals, and Achieving Health, Wealth, Happiness and Success!Rating: 5 out of 5 stars5/5 (284)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- For Women Only, Revised and Updated Edition: What You Need to Know About the Inner Lives of MenFrom EverandFor Women Only, Revised and Updated Edition: What You Need to Know About the Inner Lives of MenRating: 4.5 out of 5 stars4.5/5 (271)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- My Little Brother: The unputdownable, page-turning psychological thriller from Diane SaxonFrom EverandMy Little Brother: The unputdownable, page-turning psychological thriller from Diane SaxonRating: 4.5 out of 5 stars4.5/5 (38)
- 369: Manifesting Through 369 and the Law of Attraction - METHODS, TECHNIQUES AND EXERCISESFrom Everand369: Manifesting Through 369 and the Law of Attraction - METHODS, TECHNIQUES AND EXERCISESRating: 5 out of 5 stars5/5 (50)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (393)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Summary of The Art of Seduction by Robert GreeneFrom EverandSummary of The Art of Seduction by Robert GreeneRating: 4 out of 5 stars4/5 (46)
- The Secret Teachings Of All Ages: AN ENCYCLOPEDIC OUTLINE OF MASONIC, HERMETIC, QABBALISTIC AND ROSICRUCIAN SYMBOLICAL PHILOSOPHYFrom EverandThe Secret Teachings Of All Ages: AN ENCYCLOPEDIC OUTLINE OF MASONIC, HERMETIC, QABBALISTIC AND ROSICRUCIAN SYMBOLICAL PHILOSOPHYRating: 4.5 out of 5 stars4.5/5 (4)