You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
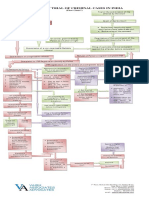
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 pageProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- Untitled PresentationDocument23 pagesUntitled Presentationapi-543394268No ratings yet
- BBC Focus - Answers To Lifes Big Questions 2017Document100 pagesBBC Focus - Answers To Lifes Big Questions 2017AD StrategoNo ratings yet
- 39 Storey Treehouse Activity Pack PDFDocument11 pages39 Storey Treehouse Activity Pack PDFNeptune Shell0% (3)
- Beacon Explorer B Press KitDocument36 pagesBeacon Explorer B Press KitBob AndrepontNo ratings yet
- Pineapple Working PaperDocument57 pagesPineapple Working PaperAnonymous EAineTiz100% (7)
- Charging Station Location and Sizing For Electric Vehicles Under CongestionDocument20 pagesCharging Station Location and Sizing For Electric Vehicles Under CongestionJianli ShiNo ratings yet
- Soal Dan Pembahasan Grammar Lat TOEP 1Document6 pagesSoal Dan Pembahasan Grammar Lat TOEP 1Abdur100% (2)
- Siy Cong Bien Vs HSBCDocument2 pagesSiy Cong Bien Vs HSBCMJ Decolongon100% (1)
- Treason Cases Digested (Crim Law 2)Document5 pagesTreason Cases Digested (Crim Law 2)Jacob Castro100% (2)
- Stock Market Prediction Using Machine Learning ProposalDocument10 pagesStock Market Prediction Using Machine Learning ProposalBilal AhmedNo ratings yet
- Speakers Reaction PaperDocument2 pagesSpeakers Reaction Papermaui100% (2)
- 9701 w19 QP 21 PDFDocument12 pages9701 w19 QP 21 PDFFaiza KhalidNo ratings yet
- ShowBoats International (May 2016)Document186 pagesShowBoats International (May 2016)LelosPinelos123100% (1)
- Rice and Contract TermsDocument7 pagesRice and Contract TermsMilling and Grain magazineNo ratings yet
- SMEC01 CBRS Guide For NBC Reports - v1.1Document53 pagesSMEC01 CBRS Guide For NBC Reports - v1.1phal sovannarithNo ratings yet
- 5 Miranda Catacutan Vs PeopleDocument4 pages5 Miranda Catacutan Vs PeopleMetoi AlcruzeNo ratings yet
- Flex Li3 21 VAADocument1 pageFlex Li3 21 VAAAyman Al-YafeaiNo ratings yet
- Feature Fusion Based On Convolutional Neural Netwo PDFDocument8 pagesFeature Fusion Based On Convolutional Neural Netwo PDFNguyễn Thành TânNo ratings yet
- QuizDocument15 pagesQuizGracie ChongNo ratings yet
- M6 - Deductions P3 (13B) Students'Document56 pagesM6 - Deductions P3 (13B) Students'micaella pasionNo ratings yet
- Form 5 A PreviewDocument4 pagesForm 5 A PreviewVikram SinghNo ratings yet
- Personal Details: Your Application Form Has Been Submitted Successfully. Payment Is SuccessfulDocument6 pagesPersonal Details: Your Application Form Has Been Submitted Successfully. Payment Is SuccessfulKanchanNo ratings yet
- USA V Meng Letter DPADocument3 pagesUSA V Meng Letter DPAFile 411No ratings yet
- MEM Companion Volume Implementation Guide - Release 1.1Document23 pagesMEM Companion Volume Implementation Guide - Release 1.1Stanley AlexNo ratings yet
- Atf Fire Research Laboratory - Technical Bulletin 02 0Document7 pagesAtf Fire Research Laboratory - Technical Bulletin 02 0Mauricio Gallego GilNo ratings yet
- Everyday Use AnalysisDocument8 pagesEveryday Use AnalysisThe 3d PlanetNo ratings yet
- 7 Types of English Adjectives That Every ESL Student Must KnowDocument3 pages7 Types of English Adjectives That Every ESL Student Must KnowBenny James CloresNo ratings yet
- Symbol Table Design (Compiler Construction)Document33 pagesSymbol Table Design (Compiler Construction)Tech_MX100% (1)
- Climate Change Forests and Forest Management An O-Wageningen University and Research 481068Document145 pagesClimate Change Forests and Forest Management An O-Wageningen University and Research 481068gulnuromar034No ratings yet