You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Kriging: Fitting A Variogram ModelDocument3 pagesKriging: Fitting A Variogram ModelAwal SyahraniNo ratings yet
- 100 PML's Tips and TricksDocument28 pages100 PML's Tips and TricksPrashant Prakash Uparkar100% (5)
- ISO 15184 Paint Hardness TesterDocument6 pagesISO 15184 Paint Hardness TesterAvinash SilimkarNo ratings yet
- Essentials of HRM - AssignmentDocument9 pagesEssentials of HRM - AssignmentAkshatNo ratings yet
- Proofs of ConspiracyDocument412 pagesProofs of Conspiracyironmercury50% (2)
- Tintas Textiles: Texiplast® - Ecofriendly Plastisols (TXP)Document180 pagesTintas Textiles: Texiplast® - Ecofriendly Plastisols (TXP)VictorSsantosNo ratings yet
- 1.4 Case Study - The Cost of Poor Communication - Technical Writing EssentialsDocument8 pages1.4 Case Study - The Cost of Poor Communication - Technical Writing EssentialssnehaashujiNo ratings yet
- COSTECH Accelration of Innovation ImbejuDocument42 pagesCOSTECH Accelration of Innovation Imbejuhamidumajid033No ratings yet
- Electric VehiclesDocument15 pagesElectric VehiclesJai ChawlaNo ratings yet
- Test BankDocument14 pagesTest BankB1111815167 WSBNo ratings yet
- LR1160 SN134056 Technical Diagrams - EnglishDocument197 pagesLR1160 SN134056 Technical Diagrams - EnglishВиталий РогожинскийNo ratings yet
- Field Trip 2 - Coreslab Structures Inc Essay - FinalDocument11 pagesField Trip 2 - Coreslab Structures Inc Essay - Finalmmg009No ratings yet
- Summary of Jordan Peterson's Biblical LecturesDocument25 pagesSummary of Jordan Peterson's Biblical LecturesRufus_DinaricusNo ratings yet
- Economic Impact of Food Culture and History of West Bengal On TouristDocument17 pagesEconomic Impact of Food Culture and History of West Bengal On Touristhitesh mendirattaNo ratings yet
- The Surgical Suture: Miriam Byrne, MD, FRCS (Plast) and Al Aly, MD, FACSDocument6 pagesThe Surgical Suture: Miriam Byrne, MD, FRCS (Plast) and Al Aly, MD, FACSRiku KusanagiNo ratings yet
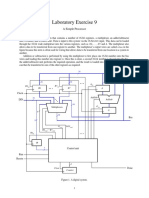
- Laboratory Exercise 9: A Simple ProcessorDocument8 pagesLaboratory Exercise 9: A Simple ProcessorhxchNo ratings yet
- B603 Series Users Manual PDFDocument36 pagesB603 Series Users Manual PDFVina MainNo ratings yet
- European Summary Report On CHP Support SchemesDocument33 pagesEuropean Summary Report On CHP Support SchemesioanitescumihaiNo ratings yet
- Kyrin Trapp 1st Grade Language Arts Lesson PlanDocument4 pagesKyrin Trapp 1st Grade Language Arts Lesson PlanKyrin TrappNo ratings yet
- AppoloDocument2 pagesAppoloRishabh Madhu SharanNo ratings yet
- School Form 1 SF 1 10Document6 pagesSchool Form 1 SF 1 10ALEX SARAOSOSNo ratings yet
- STP Model Marketing StrategyDocument25 pagesSTP Model Marketing StrategyRishab ManochaNo ratings yet
- ASA-RAC Application GuideDocument15 pagesASA-RAC Application GuideIsrael Miranda Zamarca100% (2)
- Strategies in Teaching Social Studies Inductive and Deductive Andragogy vs. PedagogyDocument31 pagesStrategies in Teaching Social Studies Inductive and Deductive Andragogy vs. PedagogyArvie VillegasNo ratings yet
- Legal CapacityDocument7 pagesLegal CapacityAreej UmerNo ratings yet
- NTFS File System Report with 25244 FilesDocument1,064 pagesNTFS File System Report with 25244 FilesAdenillson PeruannoNo ratings yet
- Inclusion/Exclusion PrincipleDocument6 pagesInclusion/Exclusion Principlekeelia1saNo ratings yet
- Mrs Jenny obstetric historyDocument3 pagesMrs Jenny obstetric historyDwi AnggoroNo ratings yet
- The Archaeology of Maritime Landscapes 2011Document363 pagesThe Archaeology of Maritime Landscapes 2011Adriana BernalNo ratings yet
- Senior Executive Assistant ResumeDocument8 pagesSenior Executive Assistant Resumef5e28dkq100% (2)