You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Step LadderExpansive Cranioplasty Mathametical ModelDocument7 pagesStep LadderExpansive Cranioplasty Mathametical ModelDebashree SenguptaNo ratings yet
- Scoring Tables EDSSDocument1 pageScoring Tables EDSSHugo Zúñiga UtorNo ratings yet
- Neuromyelitis Optica Spectrum DIsorder and Other Non-Multiple Sclerosis Central Nervous System Inflammatory DIseasesDocument30 pagesNeuromyelitis Optica Spectrum DIsorder and Other Non-Multiple Sclerosis Central Nervous System Inflammatory DIseasesnight.shadow100% (1)
- Daftar Pustaka Tumor OtakDocument2 pagesDaftar Pustaka Tumor OtakJulia Kasab 1No ratings yet
- Psych Ass ReviewerDocument3 pagesPsych Ass ReviewerPINEDA, Maria Fatima D.No ratings yet
- Centenary Ch4Document12 pagesCentenary Ch4ferisiswonoNo ratings yet
- Epidemiologija, Etiologija, Klasifikacija, Dijagnoza, Diferencijalna Dijagnoza I Tretman DemencijaDocument7 pagesEpidemiologija, Etiologija, Klasifikacija, Dijagnoza, Diferencijalna Dijagnoza I Tretman DemencijaInes StrenjaNo ratings yet
- Pediatric Demyelinating Diseases of The Central Nervous System and Their MimicsDocument338 pagesPediatric Demyelinating Diseases of The Central Nervous System and Their MimicsVu Hoang100% (1)
- Brown Séquard SyndromeDocument4 pagesBrown Séquard SyndromeDKANo ratings yet
- HBSE 3303 Dysarthria & ApraxiaDocument4 pagesHBSE 3303 Dysarthria & ApraxiasohaimimohdyusoffNo ratings yet
- This Is An Electronic Report & Not: To Be Used For Any Legal PurposesDocument1 pageThis Is An Electronic Report & Not: To Be Used For Any Legal PurposesSarmad SahabNo ratings yet
- Adam, VDL, Juillerat, & Salmon - 2000Document25 pagesAdam, VDL, Juillerat, & Salmon - 2000Sandy KOLBASINo ratings yet
- Southeast Veterinary Neurology Neurologic Exam Form: Patient Name: Age: Gender: BreedDocument2 pagesSoutheast Veterinary Neurology Neurologic Exam Form: Patient Name: Age: Gender: BreedAndres MartinezNo ratings yet
- Cerebral PalsyDocument96 pagesCerebral PalsyRahini PaniNo ratings yet
- Overall Neuropathy Limitations Scale (ONLS) - UpToDateDocument2 pagesOverall Neuropathy Limitations Scale (ONLS) - UpToDateJose Algomas Knorecuerdo0% (1)
- Management of DysarthriaDocument204 pagesManagement of DysarthriaMadhu sudarshan Reddy100% (6)
- Reviews in Pain-2011-Orofacial Pain Multiple Choice Questions-34-6Document3 pagesReviews in Pain-2011-Orofacial Pain Multiple Choice Questions-34-6Arjun Narang100% (1)
- February Outpatient Clinics - AmbrusDocument1 pageFebruary Outpatient Clinics - Ambrusbaba ababNo ratings yet
- Pengajuan Judul Skripsi Atas Nama Intan SiregarDocument54 pagesPengajuan Judul Skripsi Atas Nama Intan SiregarIntan SiregarNo ratings yet
- WWW Rehabmeasures Org Lists RehabMeasures DispForm Aspx ID 9Document21 pagesWWW Rehabmeasures Org Lists RehabMeasures DispForm Aspx ID 9Claire BarbosaNo ratings yet
- 1st Lecture On Histology of Nervous Tissue by Dr. RoomiDocument14 pages1st Lecture On Histology of Nervous Tissue by Dr. RoomiMudassar RoomiNo ratings yet
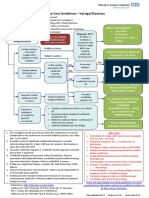
- ENT Vertigo FINAL v0.41Document1 pageENT Vertigo FINAL v0.41Farmasi BhamadaNo ratings yet
- Sound Transduction EarDocument7 pagesSound Transduction Earhsc5013100% (1)
- DR - Fouzia Batool PT - PP-DPT Lecturer, RCRSDocument48 pagesDR - Fouzia Batool PT - PP-DPT Lecturer, RCRSMuhammad Fakhar AbbasNo ratings yet
- Nerve Suply of Head and NeckDocument185 pagesNerve Suply of Head and NeckDeepika ChoudharyNo ratings yet
- What Is Gait TrainingDocument5 pagesWhat Is Gait TrainingKeyza Cose VicenteNo ratings yet
- Dapus 11 Referat 2Document3 pagesDapus 11 Referat 2Akramanto RidwanNo ratings yet
- Section 80DD, Section 80DDB, Section 80U - Tax Deduction For Disabled PersonsDocument19 pagesSection 80DD, Section 80DDB, Section 80U - Tax Deduction For Disabled Personsvvijayaraghava100% (1)
- Antiepileptic Drug QuestionsDocument2 pagesAntiepileptic Drug QuestionsFerhan AbdiNo ratings yet
- Tekle-Haimanot 1990Document15 pagesTekle-Haimanot 1990Sayak ChowdhuryNo ratings yet