You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Dermatovenereological ExamDocument3 pagesDermatovenereological ExamArya MaheswaraNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- DS Case 1 DHFDocument23 pagesDS Case 1 DHFjeboNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
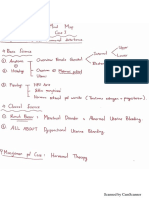
- Mind Map RPSDocument7 pagesMind Map RPSArya MaheswaraNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Basketball - Training Spring 2012Document84 pagesBasketball - Training Spring 2012Arya MaheswaraNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Tuberculosis FactsDocument8 pagesTuberculosis FactsArya MaheswaraNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Minilecture GBSDocument35 pagesMinilecture GBSArya MaheswaraNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Bahan Kuliah Myeloproliferative DisordersDocument36 pagesBahan Kuliah Myeloproliferative DisordersArya MaheswaraNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Jurnal Demam TifoidDocument5 pagesJurnal Demam TifoidLatira Lestiyani IINo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Catalog Videos APADocument28 pagesCatalog Videos APAALEJANDRO MATUTENo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Clonidine HydrochlorideDocument1 pageClonidine HydrochlorideLovelyn Joy Abubo CortezNo ratings yet
- Terapi CMLDocument7 pagesTerapi CMLAnnisa Dwi AndrianiNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- How Would We Know If Psychotherapy Were Harmful?: What Do We Mean by Harm?Document13 pagesHow Would We Know If Psychotherapy Were Harmful?: What Do We Mean by Harm?CoordinacionPsicologiaVizcayaGuaymasNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- DEMENTIADocument35 pagesDEMENTIATrixie Marie Sabile AbdullaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Non Hodgkin's Lymphoma: Rakesh BiswasDocument16 pagesNon Hodgkin's Lymphoma: Rakesh BiswasDayledaniel SorvetoNo ratings yet
- ABC FarmasiDocument34 pagesABC FarmasiOngko PriyantoNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- TizanidineDocument2 pagesTizanidinebhawanisrNo ratings yet
- Strength Training at FC Barcelona - Julio TousDocument7 pagesStrength Training at FC Barcelona - Julio Touspdelcampo1991No ratings yet
- Oral HabitsDocument78 pagesOral HabitsMrunali MaskeNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- What Is Development Guided Notes PDFDocument11 pagesWhat Is Development Guided Notes PDFMarlyn SalumbidesNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Physiomed Expert Stimulation Current Therapy - User Manual PDFDocument78 pagesPhysiomed Expert Stimulation Current Therapy - User Manual PDFpuyenkNo ratings yet
- Femoral Neck FractureDocument21 pagesFemoral Neck FractureSugar Capule - ManuelNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- SandozDocument22 pagesSandozDewa SuryaNo ratings yet
- @MBS MedicalBooksStore 2019 GettingDocument364 pages@MBS MedicalBooksStore 2019 GettingCF Ponce100% (4)
- Removable Orthodontic Appliances (ROA) 2Document83 pagesRemovable Orthodontic Appliances (ROA) 2cynjesNo ratings yet
- Spitzer 1981Document13 pagesSpitzer 1981Chima2 SantosNo ratings yet
- Sri Lakshmi Medical Centre and Hospital: 18/121 MTP Road, Thudiyalur, Coimbatore - 641 034Document49 pagesSri Lakshmi Medical Centre and Hospital: 18/121 MTP Road, Thudiyalur, Coimbatore - 641 034dhir.ankur100% (1)
- Engleza S. GingivaleDocument4 pagesEngleza S. GingivaleGeorgiana IlincaNo ratings yet
- Lab Normal Value S&Sof S&Sof : Loma Linda University School of Nursing Accepted Lab Values Adapted From KaplanDocument3 pagesLab Normal Value S&Sof S&Sof : Loma Linda University School of Nursing Accepted Lab Values Adapted From KaplanGiacen100% (3)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Respiratory Notes Sample ChapterDocument10 pagesRespiratory Notes Sample ChapterHitesh Deora75% (4)
- Franz Alexander - The Scope of PsychoanalysisDocument631 pagesFranz Alexander - The Scope of PsychoanalysisGeorge Baciu100% (1)
- Bio Electrode Therapy ManualDocument19 pagesBio Electrode Therapy ManualMokhtar Mohd100% (1)
- Fran Bruscia CVDocument5 pagesFran Bruscia CVAR GameCenterNo ratings yet
- PDF - Self-As-Context A Core Process in The ACT Hexagon ModelDocument10 pagesPDF - Self-As-Context A Core Process in The ACT Hexagon ModelErik Almeida100% (1)
- Acinetobacter Baumannii Infections UpdateDocument68 pagesAcinetobacter Baumannii Infections Updatetummalapalli venkateswara rao100% (2)
- ComputationsDocument10 pagesComputationsFaye Nervanna Alecha AlferezNo ratings yet
- Primitive ReflexesDocument6 pagesPrimitive ReflexesMarikit2012100% (1)
- Clinical Hypnosis For The Alleviation of Tinnitus: Thomas E. CopeDocument4 pagesClinical Hypnosis For The Alleviation of Tinnitus: Thomas E. CopeIsabelNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)