You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Call To ActionDocument5 pagesCall To ActionTom CotterNo ratings yet
- SunShot Vision StudyDocument320 pagesSunShot Vision StudyTom CotterNo ratings yet
- Everything Must Change - GuideDocument29 pagesEverything Must Change - GuideTom CotterNo ratings yet
- Creation Care Themes in ScriptureDocument5 pagesCreation Care Themes in ScriptureTom CotterNo ratings yet
- The Energy - Water Collison: 10 Things You Should KnowDocument6 pagesThe Energy - Water Collison: 10 Things You Should KnowTom CotterNo ratings yet
- The Hannover PrinciplesDocument59 pagesThe Hannover PrinciplesTom CotterNo ratings yet
- St. John The Devine Sermon Finakd) DumorDocument9 pagesSt. John The Devine Sermon Finakd) DumorTytyt TyyNo ratings yet
- Climate Assessment 2009 Lo RezDocument224 pagesClimate Assessment 2009 Lo RezTodd BenoitNo ratings yet
- Introduction To The Cradle To Cradle Design FrameworkDocument6 pagesIntroduction To The Cradle To Cradle Design FrameworkTom CotterNo ratings yet
- PEUGEOT 3008 HYbrid4Document21 pagesPEUGEOT 3008 HYbrid4Tom CotterNo ratings yet
- Solar FactsheetDocument2 pagesSolar FactsheetTom CotterNo ratings yet
- History of Solar EnergyDocument7 pagesHistory of Solar EnergyTom CotterNo ratings yet
- Climate Assessment 2009 Lo RezDocument224 pagesClimate Assessment 2009 Lo RezTodd BenoitNo ratings yet
- Solar and Nuclear Costs-The Historic Crossover-Solar Energy Is Now The Better BuyDocument18 pagesSolar and Nuclear Costs-The Historic Crossover-Solar Energy Is Now The Better BuyYoudont CareatallNo ratings yet
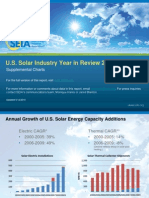
- 2009 Supplemental Charts For Solar Industry Year in ReviewDocument35 pages2009 Supplemental Charts For Solar Industry Year in ReviewTom CotterNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Generalization Quantitative Qualitative ResearchDocument8 pagesGeneralization Quantitative Qualitative ResearchLeonardo MendozaNo ratings yet
- Union College of Laguna Santa Cruz, Laguna Course Syllabus (MATH 20: Quantitative Techniques For Business)Document10 pagesUnion College of Laguna Santa Cruz, Laguna Course Syllabus (MATH 20: Quantitative Techniques For Business)RicaSanJoseNo ratings yet
- DBC011 Business Economics EMDocument338 pagesDBC011 Business Economics EMsandiNo ratings yet
- Snake and Ladder ProblemDocument8 pagesSnake and Ladder ProblemvigambetkarNo ratings yet
- BS Assignment 2: σ given, z−test, H HDocument28 pagesBS Assignment 2: σ given, z−test, H HNiharika AnandNo ratings yet
- Module 1Document41 pagesModule 1Paul Jean MerinoNo ratings yet
- Quality Control Volume 1Document182 pagesQuality Control Volume 1Saravnan Rajendran100% (3)
- 1 PBDocument10 pages1 PBMacarena Astudillo CastroNo ratings yet
- Command History 1968 Volume IIDocument560 pagesCommand History 1968 Volume IIRobert ValeNo ratings yet
- Resume 20190529Document1 pageResume 20190529Christopher DefreitasNo ratings yet
- International Journal of Advanced Trends in Computer Science and EngineeringDocument8 pagesInternational Journal of Advanced Trends in Computer Science and EngineeringLokesh AnandanNo ratings yet
- Welcome: ASM's Incon XV 10 & 11 January 2020Document22 pagesWelcome: ASM's Incon XV 10 & 11 January 2020Wency BondocNo ratings yet
- Oil & Gas UK Fire and Explosion Guidelines Issue 1 2007Document493 pagesOil & Gas UK Fire and Explosion Guidelines Issue 1 2007sorayatamara100% (4)
- 2023 - MP02 Reliability ManagementDocument88 pages2023 - MP02 Reliability ManagementOPHAR SEKTOR TAMBORANo ratings yet
- Allen 2006Document13 pagesAllen 2006Iwan Den Baguse SaputraNo ratings yet
- Chapter 1 in Work ImmersionDocument8 pagesChapter 1 in Work ImmersionLyn LomugdangNo ratings yet
- Challenges Facing Implementation of The Competency Based Curriculum in Kenya: An Urban ViewDocument14 pagesChallenges Facing Implementation of The Competency Based Curriculum in Kenya: An Urban ViewNYAMBURA NAOMINo ratings yet
- Flashlight Principles 1Document3 pagesFlashlight Principles 1kiya barrogaNo ratings yet
- Multicollinearity Correctionsv3Document2 pagesMulticollinearity Correctionsv3John NkumeNo ratings yet
- Epidemiology NotesDocument4 pagesEpidemiology Notesapi-237394422No ratings yet
- International Course: Epidemiology, Biostatistics & Qualitative Research MethodsDocument2 pagesInternational Course: Epidemiology, Biostatistics & Qualitative Research MethodsAna MarianaNo ratings yet
- ArticleDocument6 pagesArticlePakeeza JavedNo ratings yet
- 3D Surface Mapping Using Ultrasonic SensorsDocument3 pages3D Surface Mapping Using Ultrasonic SensorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chapter 1testDocument4 pagesChapter 1testLexi DavisNo ratings yet
- Chapter 7 - SPPLR Eval SelecDocument45 pagesChapter 7 - SPPLR Eval SelecAditya parmarNo ratings yet
- Example Outline For Term PaperDocument6 pagesExample Outline For Term Paperea4c954q100% (1)
- BS 1881-114 CONCRETE Density of CocreteDocument12 pagesBS 1881-114 CONCRETE Density of CocretehajimakNo ratings yet
- Fatigue Welded StructuresDocument10 pagesFatigue Welded Structuresaap1No ratings yet
- Stats Exam QnADocument9 pagesStats Exam QnApavansam6No ratings yet
- Aplication of MMN Model in Queuing Problems in Supermarkets in The Covid-19 Context PDFDocument3 pagesAplication of MMN Model in Queuing Problems in Supermarkets in The Covid-19 Context PDFNapoleonperezNo ratings yet