Professional Documents
Culture Documents
Ganong WF. Cardiovascular Homeostasis in Health and Disease
Uploaded by
M Adil AliOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Ganong WF. Cardiovascular Homeostasis in Health and Disease
Uploaded by
M Adil AliCopyright:
Available Formats
Page 1 of 1
INTRODUCTION: CARDIOVASCULAR HOMEOSTASIS IN HEALTH & DISEASE
The compensatory adjustments of the cardiovascular system to the challenges faced by the circulation normally in everyday life and abnormally in disease illustrate the integrated operation of the cardiovascular regulatory mechanisms described in the preceding chapters. The adjustments to gravity, exercise, inflammation, wound healing, shock, fainting, hypertension, and heart failure are considered in this chapter.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 1 of 5
COMPENSATIONS FOR GRAVITATIONAL EFFECTS
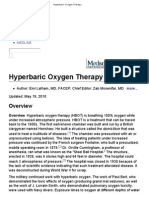
In the standing position, as a result of the effect of gravity on the blood (see Chapter 30: Dynamics of Blood & Lymph Flow), the mean arterial blood pressure in the feet of a normal adult is 180200 mm Hg and venous pressure is 8590 mm Hg. The arterial pressure at head level is 6075 mm Hg, and the venous pressure is zero. If the individual does not move, 300500 mL of blood pools in the venous capacitance vessels of the lower extremities, fluid begins to accumulate in the interstitial spaces because of increased hydrostatic pressure in the capillaries, and stroke volume is decreased. Symptoms of cerebral ischemia develop when the cerebral blood flow decreases to less than about 60% of the flow in the recumbent position. If no compensatory cardiovascular changes occurred, the reduction in cardiac output due to pooling on standing would lead to a reduction of cerebral flow of this magnitude, and consciousness would be lost. The major compensations on assuming the upright position are triggered by the drop in blood pressure in the carotid sinus and aortic arch. The heart rate increases, helping to maintain cardiac output. Relatively little venoconstriction occurs in the periphery, but there is a prompt increase in the circulating levels of renin and aldosterone. The arterioles constrict, helping to maintain blood pressure. The actual blood pressure change at heart level is variable, depending on the balance between the degree of arteriolar constriction and the drop in cardiac output (Figure 331).
Figure 331.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 2 of 5
Effect on the cardiovascular system of rising from the supine to the upright position. Figures shown are average changes. Changes in abdominal and limb resistance and in blood pressure are variable from individual to individual. (Redrawn and reproduced, with permission, from Brobeck JR [editor]: Best and Taylor's Physiological Basis of Medical Practice, 9th ed. Williams & Wilkins, 1973.)
In the cerebral circulation, additional compensatory changes take place. The arterial pressure at head level drops 2040 mm Hg, but jugular venous pressure falls 58 mm Hg, reducing the drop in perfusion pressure (arterial pressure minus venous pressure). Cerebral vascular resistance is reduced because intracranial pressure falls as venous pressure falls, decreasing the pressure on the cerebral vessels. The decline PO2 and the pH in brain tissue, further actively dilating the cerebral vessels. Because of the operation of these autoregulatory mechanisms, cerebral blood flow declines only 20% on standing. In addition, the amount of O2 extracted from each unit of in the supine and the upright positions. in cerebral blood flow increases the partial pressure of CO2 (PCO ) and decreases the
2
blood increases, and the net effect is that cerebral O2 consumption is about the same Prolonged standing presents an additional problem because of increasing interstitial fluid volume in the lower extremities. As long as the individual moves about, the
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 3 of 5
operation of the muscle pump (see Chapter 30: Dynamics of Blood & Lymph Flow) keeps the venous pressure below 30 mm Hg in the feet, and venous return is adequate. However, with prolonged quiet standing (eg, in military personnel standing at attention for long periods), fainting may result. In a sense, the fainting is a "homeostatic mechanism," because falling to the horizontal position promptly restores venous return, cardiac output, and cerebral blood flow to adequate levels. The effects of gravity on the circulation in humans depend in part upon the blood volume. When the blood volume is low, these effects are marked; when it is high, they are minimal. The compensatory mechanisms that operate on assumption of the erect posture are better developed in humans than in quadrupeds even though these animals have sensitive carotid sinus mechanisms. Quadrupeds tolerate tilting to the upright position poorly. Of course, giraffes are an exception. These long-legged animals do not develop ankle edema despite the very large increment in vascular pressure in their legs due to gravity because they have tight skin and fascia in the lower legsin a sense a built-in antigravity suit (see below)and a very effective muscle pump. Perfusion in the head is maintained by a high mean arterial pressure. When giraffes lower their heads to drink, blood is pumped up their jugular veins to the chest, presumably by rhythmic contractions of the muscles of the jaws.
Postural Hypotension
In some individuals, sudden standing causes a fall in blood pressure, dizziness, dimness of vision, and even fainting. The causes of this orthostatic postural hypotension are multiple. It is common in patients receiving sympatholytic drugs. It also occurs in diseases such as diabetes and syphilis, in which there is damage to the sympathetic nervous system. This underscores the importance of the sympathetic vasoconstrictor fibers in compensating for the effects of gravity on the circulation. Another cause of postural hypotension is primary autonomic failure (Table 331). Autonomic failure occurs in a variety of diseases. One form is caused by a congenital deficiency of dopamine -hydroxylase (see Chapter 4: Synaptic & Junctional Transmission) with little or no production of norepinephrine and epinephrine. Baroreceptor reflexes are also abnormal in patients with primary hyperaldosteronism. However, these patients generally do not have postural hypotension, because their blood volumes are expanded sufficiently to maintain cardiac output in spite of changes in position. Indeed, mineralocorticoids are used to treat patients with postural hypotension.
Table 331. Major Forms of Primary Autonomic Failure.
Bradbury-Eggleston syndrome (idiopathic orthostatic hypotension) Onset late in life Sympathetic and parasympathetic failure Absent or minimal other neurologic involvement Plasma norepinephrine/dopamine ratio greater than 1
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 4 of 5
Shy-Drager syndrome (multiple system atrophy) Onset in mid to late life Sympathetic and parasympathetic failure Other neurologic involvement (extrapyramidal, cerebellar, etc) Plasma norepinephrine/dopamine ratio greater than 1 Riley-Day syndrome (familial dysautonomia) Congenital onset and premature mortality Ashkenazi Jewish extraction Sympathetic and parasympathetic involvement Emotional lability Plasma norepinephrine/dopamine ratio greater than 1 Dopamine -hydroxylase deficiency
Congenital onset Sympathoadrenomedullary failure (orthostatic hypotension) Intact sweating Parasympathetic sparing Plasma norepinephrine/dopamine ratio much less than 1
Reproduced, with permission, from Robertson D et al: Dopamine -hydroxylase deficiency: A genetic disorder of cardiovascular regulation. Hypertension 1991;18:1. By permission of the American Heart Association, Inc.
Effects of Acceleration
The effects of gravity on the circulation are multiplied during acceleration or deceleration in vehicles that in modern civilization range from elevators to rockets. Force acting on the body as a result of acceleration is commonly expressed in g units, 1 g being the force of gravity on the earth's surface. "Positive g" is force due to acceleration acting in the long axis of the body, from head to foot; "negative g" is force due to acceleration acting in the opposite direction. During exposure to positive g, blood is "thrown" into the lower part of the body. Arterial pressure in the head is reduced, but so are venous pressure and intracranial pressure, and this reduces the decrease in arterial blood flow that would otherwise occur (see Chapter 32: Circulation Through Special Regions). Cardiac output is maintained for a time because blood is drawn from the pulmonary venous reservoir and because the force of cardiac contraction is increased. At accelerations producing more than 5 g, however, vision fails ("blackout") in about 5 seconds and unconsciousness follows almost immediately thereafter. The effects of positive g are effectively cushioned by the use of antigravity "g suits," double-walled pressure suits containing water or compressed air and regulated in such a way that they compress the abdomen and legs with a force proportionate to the positive g. This decreases venous pooling and helps maintain venous return (Figure 331).
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 5 of 5
Negative g causes increased cardiac output, a rise in cerebral arterial pressure, intense congestion of the head and neck vessels, ecchymoses around the eyes, severe throbbing head pain, and, eventually, mental confusion ("redout"). In spite of the great rise in cerebral arterial pressure, the vessels in the brain do not rupture, because generally there is an increase in intracranial pressure and their walls are supported (see Chapter 32: Circulation Through Special Regions). The tolerance for g forces exerted across the body is much greater than it is for axial g. Humans tolerate 11 g acting in a back-to-chest direction for 3 minutes and 17 g acting in a chest-toback direction for 4 minutes. Astronauts are therefore positioned to take the g forces of rocket flight in the chest-to-back direction. The tolerances in this position are sufficiently large to permit acceleration to orbital or escape velocity and deceleration back into the earth's atmosphere without ill effects.
Effects of Zero Gravity on the Cardiovascular System
From the data available to date, cardiovascular function is maintained for up to 14 months of weightlessness, though there is some disuse atrophy of the mechanisms that withstand gravity on earth. On return to earth, astronauts have postural hypotension, but this disappears and readaptation to gravity appears to be complete in 47 weeks. Of course, longer exposure to weightlessness might be a bigger problem.
Other Effects of Zero Gravity
Muscular effort is much reduced when objects to be moved are weightless, and the decrease in the extensive normal proprioceptive input due to the action of gravity on the body leads to flaccidity and atrophy of skeletal muscles. A program of regular exercises against resistance, eg, pushing against a wall or stretching a heavy rubber band, appears to decrease the loss of muscle. However, the compensation is incomplete. Other changes produced by exposure to space flight include space motion sickness (see Chapter 9: Hearing & Equilibrium), a problem that has proved to be of greater magnitude than initially expected; loss of plasma volume, probably because of headward shift of body fluids, with subsequent diuresis; loss of muscle mass; steady loss of bone mineral, with increased Ca2+ excretion; loss of red-cell mass; and alterations in plasma lymphocytes. The loss of body Ca2+ is equivalent to 0.4% of the total body Ca2+ per month, and although some evidence suggests that the loss tapers off during prolonged space flight, loss at this rate might create problems of appreciable magnitude if continued for more than 14 months. A high-calcium diet helps overcome this problem, but no totally effective treatment has yet been developed. The psychological problems associated with the isolation and monotony of prolonged space flight are also a matter of concern.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 1 of 7
EXERCISE
Exercise is associated with very extensive alterations in the circulatory and respiratory systems. For convenience, the circulatory adjustments are considered in this chapter and the respiratory adjustments in Chapter 37: Respiratory Adjustments in Health & Disease. However, it should be emphasized that they occur together in an integrated fashion as part of the homeostatic responses that make moderate to severe exercise possible.
Muscle Blood Flow
The blood flow of resting skeletal muscle is low (24 mL/100 g/min). When a muscle contracts, it compresses the vessels in it if it develops more than 10% of its maximal tension (Figure 332); when it develops more than 70% of its maximal tension, blood flow is completely stopped. Between contractions, however, flow is so greatly increased that blood flow per unit of time in a rhythmically contracting muscle is increased as much as 30-fold. Blood flow sometimes increases at or even before the start of exercise, so the initial rise is probably a neurally mediated response. Impulses in the sympathetic vasodilator system (see Chapter 31: Cardiovascular Regulatory Mechanisms) may be involved. The blood flow in resting muscle doubles after sympathectomy, so some decrease in tonic vasoconstrictor discharge may also be involved. However, once exercise has started, local mechanisms maintain the high blood flow, and there is no difference in flow in normal and sympathectomized animals.
Figure 332.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 2 of 7
Blood flow through a portion of the calf muscles during rhythmic contraction. (Reproduced, with permission, from Barcroft H, Swann HJC: Sympathetic Control of Human Blood Vessels. Arnold, 1953.)
Local mechanisms maintaining a high blood flow in exercising muscle include a fall in tissue PO2, a rise in tissue PCO , and accumulation of K+ and other vasodilator 2 metabolites (see Chapter 31: Cardiovascular Regulatory Mechanisms). The temperature rises in active muscle, and this further dilates the vessels. Dilation of the arterioles and precapillary sphincters causes a 10- to 100-fold increase in the number of open capillaries. The average distance between the blood and the active cellsand dilation increases the cross-sectional area of the vascular bed, and the velocity of flow therefore decreases. The capillary pressure increases until it exceeds the oncotic pressure throughout the length of the capillaries. In addition, the accumulation of osmotically active metabolites more rapidly than they can be carried away decreases the osmotic gradient across the capillary walls. Therefore, fluid transudation into the interstitial spaces is tremendously increased. Lymph flow is also greatly increased, limiting the accumulation of interstitial fluid and in effect greatly increasing its turnover. The decreased pH and increased temperature shift the dissociation curve for hemoglobin to the right, so that more O2 is given up by the blood. The concentration affinity of hemoglobin (see Chapter 27: Circulating Body Fluids and Chapter 35: Gas Transport between the Lungs & the Tissues). The net result is an up to threefold increase in the arteriovenous O2 difference, and the transport of CO2 out of the tissue of 2,3-DPG in the red blood cells is increased, and this further decreases the O2 the distance O2 and metabolic products must diffuseis thus greatly decreased. The
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 3 of 7
is also facilitated. All of these changes combine to make it possible for the O2 consumption of skeletal muscle to increase 100-fold during exercise. An even greater increase in energy output is possible for short periods during which the energy stores are replenished by anaerobic metabolism of glucose and the muscle incurs an O2 debt (see Chapter 3: Excitable Tissue: Muscle). The overall changes in intermediary & Nutrition. K+ dilates arterioles in exercising muscle, particularly during the early part of exercise. Muscle blood flow increases to a lesser degree during exercise in K+depleted individuals, and there is a greater tendency for severe disintegration of muscle (exertional rhabdomyolysis) to occur. metabolism during exercise are discussed in Chapter 17: Energy Balance, Metabolism,
Systemic Circulatory Changes
The systemic cardiovascular response to exercise depends on whether the muscle contractions are primarily isometric or primarily isotonic with the performance of external work. With the start of an isometric muscle contraction, the heart rate rises. This increase still occurs if the muscle contraction is prevented by local infusion of a neuromuscular blocking drug. It also occurs with just the thought of performing a muscle contraction, so it is probably the result of psychic stimuli acting on the medulla oblongata. The increase is largely due to decreased vagal tone, although increased discharge of the cardiac sympathetic nerves plays some role. Within a few seconds of the onset of an isometric muscle contraction, systolic and diastolic blood pressures rise sharply. Stroke volume changes relatively little, and blood flow to the steadily contracting muscles is reduced as a result of compression of their blood vessels. The response to exercise involving isotonic muscle contraction is similar in that there is a prompt increase in heart rate but different in that a marked increase in stroke volume occurs. In addition, there is a net fall in total peripheral resistance (Figure 33 3) due to vasodilation in exercising muscles (Table 332). Consequently, systolic blood pressure rises only moderately, whereas diastolic pressure usually remains unchanged or falls. The difference in response to isometric and isotonic exercise is explained in part by the fact that the active muscles are tonically contracted during isometric exercise and consequently contribute to increased total peripheral resistance. In addition, there is a general increase in muscle sympathetic nerve activity, apparently because of a signal from the contracted muscle. However since cholinergic sympathetic vasodilation occurs in the inactive skeletal muscles, the significance of this increase is unclear.
Table 332. Cardiac Output and Regional Blood Flow in a Sedentary Man.a
Quiet Standing
Cardiac output Blood flow to: 5900
Exercise
24,000
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 4 of 7
Heart Brain Active skeletal muscle Inactive skeletal muscle Skin Kidney, liver, gastrointestinal tract, etc.
250 750 650 650 500 3100
1000 750 20,850 300 500 600
Values are mL/min at rest and during isotonic exercise at maximal oxygen uptake.
Figure 333.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 5 of 7
Effects of different levels of isotonic exercise on cardiovascular function. (Reproduced, with permission, from Berne RM, Levy MN: Cardiovascular Physiology, 5th ed. Mosby, 1986.)
Cardiac output is increased during isotonic exercise to values that may exceed 35 L/min, the amount being proportionate to the increase in O2 consumption. The mechanisms responsible for this increase are discussed above and in Chapter 29: The Heart As a Pump. The maximal heart rate achieved during exercise decreases with age. In children, it rises to 200 or more beats per minute; in adults it rarely exceeds 195 beats per minute, and in elderly individuals the rise is even smaller. A great increase in venous return takes place, although the increase in venous return is not the primary cause of the increase in cardiac output. Venous return is increased by the great increase in the activity of the muscle and thoracic pumps; by mobilization of blood from the viscera; by increased pressure transmitted through the dilated arterioles to the veins; and by noradrenergically mediated venoconstriction, which decreases the volume of blood in the veins. The amount of blood mobilized from the splanchnic area and other reservoirs may increase the amount of blood in the arterial portion of the circulation by as much as 30% during strenuous exercise. After exercise, the blood pressure may transiently drop to subnormal levels, presumably because accumulated metabolites keep the muscle vessels dilated for a short period. However, the blood pressure soon returns to the preexercise level. The heart rate returns to normal more slowly.
Temperature Regulation
The quantitative aspects of heat dissipation during exercise are summarized in Figure 334. In many locations, the skin is supplied by branches of muscle arteries, so that some of the blood warmed in the muscles is transported directly to the skin, where some of the heat is radiated to the environment. There is a marked increase in ventilation (see Chapter 37: Respiratory Adjustments in Health & Disease), and some heat is lost in the expired air. The body temperature rises, and the hypothalamic centers that control heat-dissipating mechanisms are activated. The temperature increase is due at least in part to the inability of the heat-dissipating mechanism to handle the great increase in heat production. Sweat secretion is greatly increased, and vaporization of this sweat is the major path for heat loss. The cutaneous vessels also dilate. This dilation is primarily due to inhibition of vasoconstrictor tone, although local release of vasodilator polypeptides may also contribute (see Chapter 31: Cardiovascular Regulatory Mechanisms).
Figure 334.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 6 of 7
Energy exchange in muscular exercise. The shaded area represents the excess of heat production over heat loss. The total energy output equals the heat production plus the work done.
Training
Both at rest and at any given level of exercise, trained athletes have a larger stroke volume and lower heart rate than untrained individuals (see Chapter 29: The Heart As a Pump), and they tend to have larger hearts. Training increases the maximal oxygen consumption (VO2max) that can be produced by exercise in an individual. VO2max averages about 38 mL/kg/min in active healthy men and about 29 mL/kg/min in active healthy women. It is lower in sedentary individuals. VO2max is the product of
maximal cardiac output and maximal O2 extraction by the tissues, and both increase with training. The changes that occur in skeletal muscles with training include increases in the number of mitochondria and the enzymes involved in oxidative metabolism. The number of capillaries increases, with better distribution of blood to the muscle fibers. load, less increase in lactate production. The increase in blood flow to muscles is less and, because of this, less increase in heart rate and cardiac output than in an untrained individual. This is one of the reasons that exercise is of benefit to patients with heart disease. The net effect is more complete extraction of O2 and consequently, for a given work
Relation to Cardiovascular Disease
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 7 of 7
It is said that the internist's mantra for cardiovascular health is, "Stop smoking, lose weight, and get more exercise." The beneficial effects of a program of regular isotonic exercise are well established in terms of helping patients to feel better, have less severe heart attacks when they have them, and avoid heart attacks in the first place. Regular exercise improves coronary perfusion apparently because the exercise through shear stress improves the production of prostacyclin and NO by the endothelium of the coronary vessels. On the other hand, it is also true that the incidence of heart attacks increases during and up to 30 minutes after heavy exercise, particularly in individuals leading sedentary lives. The cause of the increase is unknown but may be related to increased rupture of atherosclerotic plaques. The long-term benefits of exercise probably outweigh the short-term dangers, but it is important to start an exercise program gradually and not let it become too strenuous.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 1 of 4
INFLAMMATION & WOUND HEALING
Local Injury
Inflammation is a complex localized response to foreign substances such as bacteria or in some instances to internally produced substances. It includes a sequence of reactions initially involving cytokines, neutrophils, adhesion molecules, complement, and IgG. PAF, an agent with potent inflammatory effects (see Chapter 27: Circulating Body Fluids), also plays a role. Later, monocytes and lymphocytes are involved. Arterioles in the inflamed area dilate, and capillary permeability is increased (see Chapter 31: Cardiovascular Regulatory Mechanisms and Chapter 32: Circulation Through Special Regions). When the inflammation occurs in or just under the skin (Figure 335), it is characterized by redness, swelling, tenderness, and pain. Elsewhere, it is a key component of asthma, ulcerative colitis, and many other diseases.
Figure 335.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 2 of 4
Cutaneous wound 3 days after injury, showing the multiple cytokines and growth factors affecting the repair process. VEGF, vascular endothelial growth factor. For other abbreviations, see Appendix. Note the epidermis growing down under the fibrin clot, restoring skin continuity. (Modified from Singer AJ, Clark RAF: Cutaneous wound healing. N Engl J Med 1999;341:738.)
Evidence is accumulating that a transcription factor, nuclear factor- B, plays a key role in the inflammatory response. NF- B is a heterodimer that normally exists in the cytoplasm of cells bound to I B , which renders it inactive. Stimuli such as cytokines, viruses, and oxidants separate NF- B from I B , which is then degraded. NF- B moves to the nucleus, where it binds to the DNA of the genes for numerous inflammatory mediators, resulting in their increased production and secretion. Glucocorticoids inhibit the activation of NF- B by increasing the production of I B , and this is probably the main basis of their antiinflammatory action (see Chapter 20: The Adrenal Medulla & Adrenal Cortex).
Systemic Response to Injury
Cytokines produced in response to inflammation and other injuries also produce systemic responses. These include alterations in plasma acute phase proteins, defined as proteins whose concentration is increased or decreased by at least 25% following injury. Many of the proteins are of hepatic origin and are listed in Table 27 9. A number of them are shown in Figure 336. The causes of the changes in concentration are incompletely understood, but it can be said that many of the changes make homeostatic sense. Thus, for example, an increase in C-reactive protein activates monocytes and causes further production of cytokines.
Figure 336.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 3 of 4
Time course of changes in some major acute phase proteins. C3, C3 component of complement. (Modified and reproduced with permission, from Gitlin JD, Colten HR: Molecular biology of acute phase plasma proteins. In Pick F et al [editors]. Lymphokines, vol 14, pages 123153. Academic Press, 1987.)
Other changes that occur in response to injury include somnolence, negative nitrogen balance, and fever.
Wound Healing
When tissue is damaged, platelets adhere to exposed matrix via integrins that bind to collagen and laminin (Figure 335). Blood coagulation produces thrombin, which promotes platelet aggregation and granule release. The platelet granules generate an inflammatory response. White blood cells are attracted by selectins and bind to integrins on endothelial cells, leading to their extravasation through the blood vessel walls. Cytokines released by the white blood cells and platelets up-regulate integrins on macrophages, which migrate to the area of injury, and on fibroblasts and epithelial cells, which mediate wound healing and scar formation. Plasmin aids healing by removing excess fibrin. This aids the migration of keratinocytes into the wound to restore the epithelium under the scab. Collagen proliferates, producing the scar.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 4 of 4
Wounds gain 20% of their ultimate strength in 3 weeks and later gain more strength, but they never reach more than about 70% of the strength of normal skin.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 1 of 6
SHOCK
General Considerations
Shock is a syndrome about which there has been a great deal of confusion and controversy. Part of the difficulty lies in the loose use of the term by physiologists and physicians as well as laymen. Electric shock and spinal shock, for example, bear no relation to the condition produced by hemorrhage and related cardiovascular abnormalities. Shock in the restricted sense of "circulatory shock" is still a collection of different entities that share certain common features. However, the feature that is common to all the entities is inadequate tissue perfusion with a relatively or absolutely inadequate cardiac output. The cardiac output may be inadequate because the amount of fluid in the vascular system is inadequate to fill it (hypovolemic shock). Alternatively, it may be inadequate in the relative sense because the size of the vascular system is increased by vasodilation even though the blood volume is normal (distributive, vasogenic, or low-resistance shock). Shock may also be caused by inadequate pumping action of the heart as a result of myocardial abnormalities (cardiogenic shock), and by inadequate cardiac output as a result of obstruction of blood flow in the lungs or heart (obstructive shock). These forms of shock are listed in Table 333, along with examples of the disease processes that can cause them.
Table 333. Types of Shock, with Examples of Conditions or Diseases That Can Cause Each Type.
Hypovolemic shock (decreased blood volume) Hemorrhage Trauma Surgery Burns Fluid loss due to vomiting or diarrhea Distributive shock (marked vasodilation; also called vasogenic or low-resistance shock) Fainting (neurogenic shock) Anaphylaxis Sepsis (also causes hypovolemia due to increased capillary permeability with loss of fluid into tissues) Cardiogenic shock (inadequate output by a diseased heart) Myocardial infarction Congestive heart failure Arrhythmias Obstructive shock (obstruction of blood flow) Tension pneumothorax Pulmonary embolism Cardiac tumor Cardiac tamponade
Hypovolemic Shock
Hypovolemic shock is also called "cold shock." It is characterized by hypotension; a rapid, thready pulse; a cold, pale, clammy skin; intense thirst; rapid respiration; and restlessness or, alternatively, torpor. None of these findings, however, are invariably present. The hypotension may be relative. A hypertensive patient whose blood pressure is regularly 240/140, for example, may be in severe shock when the blood pressure is 120/90. Hypovolemic shock is commonly subdivided into categories on the basis of cause. The use of terms such as "hemorrhagic shock," "traumatic shock," "surgical shock," and "burn shock" is of some benefit because, although these various forms of shock have similarities, there are important features that are unique to each.
Hemorrhagic Shock
It is useful to consider the effects of hemorrhage in some detail because they illustrate the features of a major form of hypovolemic shock and the multiple compensatory reactions that come into play to defend ECF volume. The principal reactions are listed in Table 334.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 2 of 6
Table 334. Compensatory Reactions Activated by Hemorrhage.
Vasoconstriction Tachycardia Venoconstriction Tachypnea Restlessness increased thoracic pumping increased skeletal muscle pumping (in some cases)
Increased movement of interstitial fluid into capillaries Increased secretion of norepinephrine and epinephrine Increased secretion of vasopressin Increased secretion of glucocorticoids Increased secretion of renin and aldosterone Increased secretion of erythropoietin Increased plasma protein synthesis The decline in blood volume produced by bleeding decreases venous return, and cardiac output falls. The heart rate is increased, and with severe hemorrhage, a fall in blood pressure always occurs. With moderate hemorrhage (515 mL/kg body weight), pulse pressure is reduced but mean arterial pressure may be normal. The blood pressure changes vary from individual to individual, even when exactly the same amount of blood is lost. The skin is cool and pale and may have a grayish tinge because of stasis in the capillaries and a small amount of cyanosis. Respiration is rapid, and in patients whose consciousness is not obtunded, intense thirst is a prominent symptom. In hypovolemic and other forms of shock, the inadequate perfusion of the tissue leads to increased anaerobic glycolysis, with the production of large amounts of lactic acid. In severe cases, the blood lactate level rises from the normal value of about 1 mmol/L to 9 mmol/L or more. The resulting lactic acidosis depresses the myocardium, decreases peripheral vascular responsiveness to catecholamines, and may be severe enough to cause coma.
Rapid Compensatory Reactions
When blood volume is reduced and venous return is decreased, the arterial baroreceptors are stretched to a lesser degree and sympathetic output is increased. Even if there is no drop in mean arterial pressure, the decrease in pulse pressure decreases the rate of discharge in the arterial baroreceptors, and reflex tachycardia and vasoconstriction result. It is interesting that with more severe blood loss, tachycardia is replaced by bradycardia; this occurs while shock is still reversible (see below). With even greater hemorrhage, the heart rate rises again. The bradycardia is presumably due to unmasking a vagally mediated depressor reflex, and the response may have evolved as a mechanism for stopping further blood loss. The vasoconstriction is generalized, sparing only the vessels of the brain and heart. The vasoconstrictor innervation of the cerebral arterioles is probably insignificant from a functional point of view, and the coronary vessels are dilated because of the increased myocardial metabolism secondary to the increase in heart rate (see Chapter 32: Circulation Through Special Regions). Vasoconstriction is most marked in the skin, where it accounts for the coolness and pallor, and in the kidneys and viscera. Hemorrhage also evokes a widespread reflex venoconstriction that helps maintain the filling pressure of the heart, although the receptors that initiate the venoconstriction are unsettled. The intense vasoconstriction in the splanchnic area shifts blood from the visceral reservoir into the systemic circulation. Blood is also shifted out of the subcutaneous and pulmonary veins. Contraction of the spleen discharges more "stored" blood into the circulation, although the volume mobilized in this way in humans is small. In the kidneys, both afferent and efferent arterioles are constricted, but the efferent vessels are constricted to a greater degree. The glomerular filtration rate is depressed, but renal plasma flow is decreased to a greater extent, so that the filtration fraction (glomerular filtration rate divided by renal plasma flow) increases. Na+ retention is marked, and the nitrogenous products of metabolism are retained in the blood (azotemia or uremia). Especially when the hypotension is prolonged, renal tubular damage may be severe (acute renal failure). Hemorrhage is a potent stimulus to adrenal medullary secretion (see Chapter 20: The Adrenal Medulla & Adrenal Cortex). Circulating norepinephrine is also increased because of the increased discharge of sympathetic noradrenergic neurons. The increase in circulating catecholamines probably contributes relatively little to the generalized vasoconstriction, but it may lead to stimulation of the reticular formation (see Chapter 11: Alert Behavior, Sleep, & the Electrical Activity of the Brain). Possibly because of such reticular stimulation, some patients in hemorrhagic shock are restless and apprehensive. Others are quiet and apathetic, and their sensorium is dulled, probably because of cerebral ischemia and acidosis. When restlessness is present, increased motor activity and
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 3 of 6
increased respiratory movements increase the muscular and thoracic pumping of venous blood. The loss of red cells decreases the O2-carrying power of the blood, and the blood flow in the carotid and aortic
bodies is reduced. The resultant anemia and stagnant hypoxia (see Chapter 37: Respiratory Adjustments in Health &
Disease), as well as the acidosis, stimulate the chemoreceptors. Increased activity in chemoreceptor afferents is probably the main cause of respiratory stimulation in shock. Chemoreceptor activity also excites the vasomotor areas in the medulla, increasing vasoconstrictor discharge. In fact, in hemorrhaged dogs with arterial pressures of less than 70 mm Hg, cutting the nerves to the carotid baroreceptors and chemoreceptors may cause a further fall in blood pressure rather than a rise. This paradoxic result occurs because no baroreceptor discharge takes place at pressures below 70 mm Hg, and activity in fibers from the carotid chemoreceptors is driving the vasomotor area beyond the maximal rate produced by release of baroreceptor inhibition. The increase in the level of circulating angiotensin II produced by the increase in plasma renin activity during hemorrhage causes thirst by an action on the subfornical organ (see Chapter 32: Circulation Through Special Regions), and ingestion of fluid helps restore the ECF volume. The increase in angiotensin II also helps to maintain blood pressure. The blood pressure fall produced by removal of a given volume of blood is greater in animals infused with drugs that block angiotensin II receptors than it is in controls. Vasopressin also raises blood pressure when administered in large doses in normal animals, but infusion of doses that produce the same plasma vasopressin levels produced by hemorrhage causes only a small increase in blood pressure because a compensatory decrease in cardiac output occurs (see Chapter 31: Cardiovascular Regulatory Mechanisms). However, blood pressure falls when peptides that antagonize the effects of vasopressin are injected following hemorrhage. Thus, it appears that vasopressin also plays a significant role in maintaining blood pressure. The increases in circulating angiotensin II and ACTH levels increase aldosterone secretion, and the increased circulating levels of aldosterone and vasopressin cause retention of Na+ and water, which helps reexpand the blood volume. However, aldosterone takes about 30 minutes to exert its effect, and the initial decline in urine volume and Na+ excretion is certainly due for the most part to the hemodynamic alterations in the kidney. When the arterioles constrict and the venous pressure falls because of the decrease in blood volume, a drop in capillary pressure takes place. Fluid moves into the capillaries along most of their course, helping to maintain the circulating blood volume. This decreases interstitial fluid volume, and fluid moves out of the cells.
Long-Term Compensatory Reactions
After a moderate hemorrhage, the circulating plasma volume is restored in 1272 hours (Figure 337). Preformed albumin also enters rapidly from extravascular stores, but most of the tissue fluids that are mobilized are proteinfree. They dilute the plasma proteins and cells, but when whole blood is lost, the hematocrit may not fall for several hours after the onset of bleeding. After the initial influx of preformed albumin, the rest of the plasma protein losses are replaced, presumably by hepatic synthesis, over a period of 34 days. Erythropoietin appears in the circulation, and the reticulocyte count increases, reaching a peak in 10 days. The red cell mass is restored to normal in 48 weeks. However, a low hematocrit is remarkably well tolerated because of various compensatory mechanisms. One of these is an increase in the concentration of 2,3-BPG in the red blood cells, which causes hemoglobin to give more O2 to the tissues (see Chapter 27: Circulating Body Fluids). In long-standing anemia in otherwise healthy individuals, exertional dyspnea is not observed until the hemoglobin concentration is about 7.5 g/dL. Weakness becomes appreciable at about 6 g/dL; dyspnea at rest appears at about 3 g/dL; and the heart fails when the hemoglobin level falls to 2 g/dL.
Figure 337.
Changes in red cell volume (dark color), plasma volume (light color), and total plasma protein following hemorrhage in a
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 4 of 6
normal human subject.
Refractory Shock
Depending largely on the amount of blood lost, some patients die soon after hemorrhage and others recover as the compensatory mechanisms, aided by appropriate treatment, gradually restore the circulation to normal. In an intermediate group of patients, shock persists for hours and gradually progresses to a state in which no response to vasopressor drugs takes place and in which, even if the blood volume is returned to normal, cardiac output remains depressed. This is known as refractory shock. The condition is not unique to hemorrhagic shock but occurs in other forms as well. It used to be called irreversible shock, and patients still do die despite vigorous treatment. However, more and more patients are saved as understanding of the pathophysiologic mechanisms increases and treatment improves. Therefore, refractory shock seems to be a more appropriate term. Various positive feedback mechanisms contribute to the production of refractory shock. For example, severe cerebral ischemia leads eventually to depression of the vasomotor and cardiac areas of the brain, causing vasodilation and reduction of the heart rate. These both make the blood pressure drop further, with a further reduction in cerebral blood flow and further depression of the vasomotor and cardiac areas. Another important example of this type of positive feedback is myocardial depression. In severe shock, the coronary blood flow is reduced because of the hypotension and tachycardia (see Chapter 32: Circulation Through Special Regions), even though the coronary vessels are dilated. The myocardial failure makes the shock and the acidosis worse, and this in turn leads to further depression of myocardial function. If the reduction is marked and prolonged, the myocardium may be damaged to the point where cardiac output cannot be restored to normal in spite of reexpansion of the blood volume. A late complication of shock that can be fatal is pulmonary damage with the production of acute respiratory distress syndrome (ARDS, adult respiratory distress syndrome; see Chapter 37: Respiratory Adjustments in Health & Disease). This syndrome is characterized by acute respiratory failure with a high mortality, and it can be triggered not only by shock but also by sepsis, lung contusion, other forms of trauma, and other serious conditions. The common feature seems to be damage to capillary endothelial cells and alveolar epithelial cells, with release of cytokines.
Other Forms of Hypovolemic Shock
Traumatic shock develops when muscle and bone are severely damaged. This is the type of shock seen in battle casualties and automobile accident victims. Frank bleeding into the injured areas is the principal cause of the shock, although some plasma also enters the tissue. The amount of blood which can be lost into an injury that appears relatively minor is remarkable; the thigh muscles can accommodate 1 L of extravasated blood, for example, with an increase in the diameter of the thigh of only 1 cm. Breakdown of skeletal muscle (rhabdomyolysis) is a serious additional problem when shock is accompanied by extensive muscle crushing (crush syndrome). Kidney damage is also common in the crush syndrome. It is due to accumulation of myoglobin and other products from reperfused tissue in kidneys in which glomerular filtration is already reduced by shock. The products damage and clog the tubules, frequently causing anuria, which may be fatal. Surgical shock is due to the combination in various proportions of external hemorrhage, bleeding into injured tissues, and dehydration. In burn shock, the most apparent abnormality is loss of plasma as exudate from the burned surfaces. Since the loss in this situation is plasma rather than whole blood, the hematocrit rises and hemoconcentration is a prominent finding. Burns also cause complex, poorly understood metabolic changes in addition to fluid loss. For example, the metabolic rate of nonthyroidal origin rises by 50%, and some burned patients develop hemolytic anemia. Because of these complications, plus the severity of the shock and the problems of sepsis and kidney damage, the mortality rate when third-degree burns cover more than 75% of the body is still close to 100%. Hypovolemic shock is a complication of various metabolic and infectious diseases. For example, although the mechanism is different in each case, adrenal insufficiency, diabetic ketoacidosis, and severe diarrhea are all characterized by loss of Na+ from the circulation. The resultant decline in plasma volume may be severe enough to precipitate cardiovascular collapse.
Distributive Shock
As noted above, distributive shock occurs when the blood volume is normal but the capacity of the circulation is increased by marked vasodilation. It is also called "warm shock" because the skin is not cold and clammy, as it is in hypovolemic shock. A good example is anaphylactic shock, a rapidly developing, severe allergic reaction that
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 5 of 6
sometimes occurs when an individual who has previously been sensitized to an antigen is reexposed to it. The resultant antigenantibody reaction releases large quantities of histamine, causing increased capillary permeability and widespread dilation of arterioles and capillaries.
Septic Shock
Septic shock is a common and serious condition in which infections, usually due to gram-negative bacteria, cause shock which has both distributive and hypovolemic features. Endotoxins, the cell wall lipopolysaccharides produced by some bacteria, cause vasodilation and increased capillary permeability, with loss of plasma in the tissues. They also initiate a complex series of cytokine and coagulant reactions that can lead eventually to multiple organ failure. The mortality of the condition is 3050%, and numerous drugs designed to inhibit the inflammatory response, including glucocorticoids have failed to lower this figure. However, promising results have been obtained with activated protein C, which has anticoagulant activity (see Chapter 27: Circulating Body Fluids).
Fainting
A third type of distributive shock is neurogenic shock, in which a sudden burst of autonomic activity produces vasodilation, pooling of blood in the extremities, and fainting. These are called vasovagal attacks, and they are short-lived and benign. Other forms of syncope include postural syncope, fainting due to pooling of blood in the dependent parts of the body on standing. Micturition syncope, fainting during urination, occurs in patients with orthostatic hypotension. It is due to the combination of the orthostasis and reflex bradycardia induced by voiding in these patients. Pressure on the carotid sinus, produced, for example, by a tight collar, can cause such marked bradycardia and vasodilation that fainting results (carotid sinus syncope). Rarely, vasodilation and bradycardia may be precipitated by swallowing (deglutition syncope). Cough syncope occurs when the increase in intrathoracic pressure during straining or coughing is sufficient to block venous return. Effort syncope is fainting on exertion as a result of inability to increase cardiac output to meet the increased demands of the tissues and is particularly common in patients with aortic or pulmonary stenosis. Syncope can also be due to more serious abnormalities. About 25% of syncopal episodes are of cardiac origin and are due to either transient obstruction of blood flow through the heart or sudden decreases in cardiac output owing to various cardiac arrhythmias. Fainting due to bradycardia, heart block, or sinus arrest is called neurocardiogenic syncope. In addition, fainting is the presenting symptom in 7% of patients with myocardial infarctions. Thus, all cases of syncope should be investigated to determine the cause.
Cardiogenic & Obstructive Shock
When the pumping function of the heart is impaired to the point that blood flow to the tissues is no longer adequate to meet resting metabolic demands, the condition that results is called cardiogenic shock. It is most commonly due to extensive infarction of the left ventricle, but it can also be caused by other diseases that severely compromise ventricular function. The symptoms are those of shock plus congestion of the lungs and viscera because the heart fails to put out all the venous blood returned to it. Consequently, the condition is sometimes called "congested shock." The incidence of this shock in patients with myocardial infarction is about 10%, and it has a mortality of 60 90%. The picture of congested shock is also seen in obstructive shock. When the obstruction is due to tension pneumothorax with kinking of the great veins (see Chapter 37: Respiratory Adjustments in Health & Disease) or bleeding into the pericardium with external pressure on the heart (cardiac tamponade), prompt surgical intervention is required to prevent death.
Treatment of Shock
The treatment of shock should be aimed at correcting the cause and helping the physiologic compensatory mechanisms to restore an adequate level of tissue perfusion. In hemorrhagic, traumatic, and surgical shock, for example, the primary cause of the shock is blood loss, and the treatment should include early and rapid transfusion of adequate amounts of compatible whole blood. Saline is of limited temporary value. The immediate goal is restoration of an adequate circulating blood volume, and since saline is distributed in the ECF, only 25% of the amount administered stays in the vascular system. In burn shock and other conditions in which there is hemoconcentration, plasma is the treatment of choice to restore the fundamental defect, the loss of plasma. "Plasma expanders," solutions of sugars of high molecular weight and related substances that do not cross capillary walls, have some merit. Concentrated human serum albumin and other hypertonic solutions expand the blood volume by drawing fluid out of the interstitial spaces. They are valuable in emergency treatment but have the disadvantage of further dehydrating the tissues of an already dehydrated patient. In anaphylactic shock, epinephrine has a highly beneficial and almost specific effect that must represent more than
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 6 of 6
just constriction of the dilated vessels.
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 1 of 4
HYPERTENSION
Hypertension is a sustained elevation of the systemic arterial pressure. Pulmonary hypertension also occurs, but the pressure in the pulmonary artery (see Chapter 34: Pulmonary Function) is relatively independent of that in the systemic arteries.
Experimental Hypertension
The arterial pressure is determined by the cardiac output and the peripheral resistance (pressure = flow x resistance; see Chapter 30: Dynamics of Blood & Lymph Flow). The peripheral resistance is determined by the viscosity of the blood and, more importantly, by the caliber of the resistance vessels. Hypertension can be produced by elevating the cardiac output, but sustained hypertension is usually due to increased peripheral resistance. Some of the procedures that have been reported to produce sustained hypertension in experimental animals are listed in Table 335. For the most part, the procedures involve manipulation of the kidneys, the nervous system, or the adrenals. In addition a number of strains of rats develop hypertension either spontaneously (SHR rats) or when fed a high-sodium diet (Dahl salt-sensitive rats).
Table 335. Procedures That Produce Sustained Hypertension in Experimental Animals.
Interference with renal blood flow (renal hypertension) Constriction of one renal artery; other kidney removed (one-clip, one-kidney Goldblatt hypertension) Constriction of one renal artery; other kidney intact (one-clip, two-kidney Goldblatt hypertension) Constriction of aorta or both renal arteries (two-clip, two-kidney Goldblatt hypertension) Compression of kidney by rubber capsules, production of perinephritis, etc Interruptions of afferent input from arterial baroreceptors (neurogenic hypertension) Denervation of carotid sinuses and aortic arch Bilateral lesions of nucleus of tractus solitarius Treatment with corticosteroids Deoxycorticosterone and salt Other mineralocorticoids Partial adrenalectomy (adrenal regeneration hypertension) Genetic Spontaneous hypertension in various strains of rats Salt-induced hypertension in genetically sensitive rats
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 2 of 4
Endothelial NOS gene knockout in mice Various types of transgenic animals The hypertension that follows constriction of the renal arterial blood supply or compression of the kidney is called renal hypertension. As noted in Chapter 24: Endocrine Functions of the Kidneys, Heart, & Pineal Gland, some animals with renal hypertension have elevated plasma renin activity, whereas others do not. In general, one-clip, two-kidney Goldblatt hypertension (Table 335) is renin-dependent, whereas one-clip, one-kidney Goldblatt hypertension is not. An additional factor that probably contributes to renal hypertension is decreased ability of the constricted kidney to excrete Na+. Neurogenic hypertension is discussed in Chapter 31: Cardiovascular Regulatory Mechanisms. Provided that salt intake is normal or high, deoxycorticosterone causes hypertension which may persist after treatment is stopped. The hypertension is more severe in unilaterally nephrectomized animals.
Hypertension in Humans
Hypertension is a very common abnormality in humans. It can be produced by many diseases (Table 336). It causes a number of serious disorders. When the resistance against which the left ventricle must pump (afterload) is elevated for a long period, the cardiac muscle hypertrophies. The initial response is activation of immediateearly genes in the ventricular muscle, followed by activation of a series of genes involved in growth during fetal life. Left ventricular hypertrophy is associated with a poor prognosis. The total O2 consumption of the heart, already increased by the work of expelling blood against a raised pressure (see Chapter 29: The Heart As a Pump), is increased further because there is more muscle. Therefore, any decrease in coronary blood flow has more serious consequences in hypertensive patients than it does in normal individuals, and degrees of coronary narrowing that do not produce symptoms when the size of the heart is normal may produce myocardial infarction when the heart is enlarged. The incidence of atherosclerosis increases in hypertension, and myocardial infarcts are common even when the heart is not enlarged. Eventually, the ability to compensate for the high peripheral resistance is exceeded, and the heart fails. Hypertensive individuals are also predisposed to thromboses of cerebral vessels and cerebral hemorrhage. An additional complication is renal failure. However, the incidence of heart failure, strokes, and renal failure can be markedly reduced by active treatment of hypertension, even when the hypertension is relatively mild.
Table 336. Estimated Frequency of Various Forms of Hypertension in the General Hypertensive Population.
Percentage of Population
Essential hypertension 88
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 3 of 4
Renal hypertension Renovascular Parenchymal Endocrine hypertension Primary aldosteronism Cushing's syndrome Pheochromocytoma Other adrenal forms Estrogen treatment ("pill hypertension") Miscellaneous (Liddle's syndrome, coarctation of the aorta, etc) 5 0.1 0.1 0.2 1 0.6 2 3
Reproduced, with permission, from McPhee SJ, Lingappa V, Ganong WF. Pathophysiology of Disease, 4th ed. McGraw-Hill, 2003.
Malignant Hypertension
Chronic hypertension can enter an accelerated phase in which necrotic arteriolar lesions develop and there is a rapid downhill course with papilledema, cerebral symptoms, and progressive renal failure. This syndrome is known as malignant hypertension, and without treatment it is fatal in less than 2 years. However, its progression can be stopped, and it can be reversed by appropriate antihypertensive therapy.
Essential Hypertension
In about 88% of patients with elevated blood pressure, the cause of the hypertension is unknown, and they are said to have essential hypertension. At present, essential hypertension is treatable but not curable. Effective lowering of the blood pressure can be produced by drugs that block -adrenergic receptors, either in the periphery or in the central nervous system; drugs that block adrenergic receptors; drugs that inhibit the activity of angiotensin-converting enzyme; and calcium channel blockers that relax vascular smooth muscle. Essential hypertension is probably polygenic in origin, and environmental factors are also involved.
Other Forms of Hypertension
In other, less common forms of hypertension, the cause is known. A review of these is helpful because it emphasizes ways disordered physiology can lead to disease. Pathology that compromises the renal blood supply leads to renal hypertension. So does narrowing (coarctation) of the thoracic aorta, which both increases renin secreation and increases peripheral resistance. Pheochromocytomas, adrenal
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 4 of 4
medullary tumors that secrete norepinephrine and epinephrine, can cause sporadic or sustained hypertension (see Chapter 20: The Adrenal Medulla & Adrenal Cortex). Estrogens increase angiotensinogen secretion, and contraceptive pills containing large amounts of estrogen cause hypertension (pill hypertension) on this basis (see Chapter 24: Endocrine Functions of the Kidneys, Heart, & Pineal Gland). Increased secretion of aldosterone or other mineralocorticoids causes renal Na+ retention, which leads to hypertension. A primary increase in plasma mineralocorticoids inhibits renin secretion. For unknown reasons, plasma renin is also low in 1015% of patients with essential hypertension and normal circulating mineralocortical levels (low renin hypertension). Mutations in a number of single genes are known to cause hypertension. These cases of monogenic hypertension are rare, but informative. One of these is glucocorticoid-remediable aldosterenism (GRA), in which a hybrid gene encodes an ACTH-sensitive aldosterone synthase, with resulting hyperaldosterenism (see Chapter 20: The Adrenal Medulla & Adrenal Cortex). Eleven- hydroxylase deficiency also causes hypertension by increasing the secretion of deoxycorticosterone (see Chapter 20: The Adrenal Medulla & Adrenal Cortex). Normal blood pressure is restored when ACTH secretion is inhibited by administering a gluccocorticoid. Mutations that decrease 11- hydroxysteroid dehydrogenase cause loss of specificity of the mineralocorticoid receptors (see Chapter 20: The Adrenal Medulla & Adrenal Cortex) with stimulation of them by cortisol and in pregnancy, by the elevated circulation levels of progesterone. Finally, mutations of the genes for ENaCs that disrupt their or subunits increase ENaC activity and lead to excess renal Na+ retention and hypertension (Liddle's syndrome; see Chapter 38: Renal Function & Micturition).
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 1 of 3
HEART FAILURE
Pathogenesis
Heart failure occurs when the heart is unable to put out an amount of blood that is adequate for the needs of the tissues. It can be acute and associated with sudden death, or chronic. The failure may involve primarily the right ventricle (cor pulmonale), but much more commonly it involves the larger, thicker left ventricle or both ventricles. In chronic heart failure (congestive heart failure), cardiac output is initially inadequate during exercise but adequate at rest (Figure 338). As the disease progresses, the output at rest also becomes inadequate. There are two types of failure, systolic and diastolic. In systolic failure, stroke volume is reduced because ventricular contraction is weak. This causes an increase in the end-systolic ventricular volume, so that the ejection fractionthe fraction of the blood in the ventricle that is ejected during systolefalls from 65% to as low as 20%. The initial response to failure is activation of the genes that cause cardiac myocytes to hypertrophy, and thicken of the ventricular wall (cardiac remodeling). The incomplete filling of the arterial system leads to increased discharge of the sympathetic nervous system and increased secretion of renin and aldosterone, so Na+ and water are retained. These responses are initially compensatory, but eventually the failure worsens and the ventricales dilate.
Figure 338.
Decreased cardiac output in congestive heart failure. R, rest; E, maximal exercise. Note that with moderate failure, resting cardiac output is normal and only the portion going to skeletal muscle during exercise is reduced. As failure progresses, resting cardiac output is also reduced. (Modified and reproduced, with permission, from Zelis R et al:
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 2 of 3
Vasoconstrictor mechanisms in congestive heart failure, Part I. Mod Concepts Cardiovasc Dis 1989;58:7. By permission of the American Heart Association, Inc.)
In diastolic failure, the ejection fraction is initially maintained but the elasticity of the myocardium is reduced so filling during diastole is reduced. This leads to inadequate stroke volume and the same cardiac remodeling and Na+ and water retention that occur in systolic failure. It should be noted that the inadequate cardiac output in failure may be relative rather than absolute. When a large arterior venous fistula is present, in thyrotoxicosis, and in thiamine deficiency, cardiac output may be elevated in absolute terms but still be inadequate to meet the needs of the tissues (high-output failure). The principal symptoms and signs of congestive failure include cardiac enlargement and the symptoms and signs listed in Table 337.
Table 337. Simplified Summary of Pathogenesis of Major Findings in Congestive Heart Failure.
Abnormality
Weakness, exercise intolerance, fatigue Ankle, sacral edema Hepatomegaly Pulmonary congestion Dyspnea on exertion Paroxysmal dyspnea, pulmonary edema Orthopnea
Cause
Left ventricle; output inadequate to perfuse muscles; especially, failure of output to rise with exercise. Increased peripheral venous pressure transudation. Increased peripheral venous pressure to portal flow. increased fluid increased resistance
Increased pulmonary venous pressure pulmonary venous distention and transudation of fluid into air spaces. Failure of left ventricular output to rise during exercise increased pulmonary venous pressure. Probably sudden failure of left heart output to keep up with right heart output acute rise in pulmonary venous and capillary pressure transudation of fluid into air spaces. Normal pooling of blood in lungs in supine position added to already congested pulmonary vascular system; increased venous return not put out by left ventricle. (Relieved by sitting up, raising head of bed, lying on extra pillows.) Greater ventricular end-diastolic volume.
Cardiac dilation
Treatment
Treatment of congestive heart failure is aimed at improving cardiac contractility, treating the symptoms, and decreasing the load on the heart. Currently, the most effective treatment in general use is inhibition of the production of angiotensin II with angiotensin-converting enzyme inhibitors. Blockade of the effects of angiotensin II on AT1 receptors with nonpeptide antagonists is also of value. Angiotensin II
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
Page 3 of 3
appears to have direct effects on the heart, although these are controversial. Blocking the production of angiotensin II or its effects also reduces the circulating aldosterone level and decreases blood pressure, reducing the afterload against which the heart pumps. The effects of aldosterone can be further reduced by administering aldosterone receptor blockers, and these have shown promise in recent trials. Reducing venous tone with nitrates or hydralazine increases venous capacity so that the amount of blood returned to the heart is reduced, lowering the preload. Diuretics reduce the fluid overload. Drugs that block -adrenergic receptors have been shown to decrease mortality and morbidity. Digitalis derivatives such as digoxin have classically been used to treat congestive failure because of their ability to increase intra-cellular Ca2+ and hence exert a positively inotropic effect (see Chapter 3: Excitable Tissue: Muscle), but they are now used in a secondary role to treat systolic dysfunction and slow the ventricular rate in patients with atrial fibrillation (see Chapter 28: Origin of the Heartbeat & the Electrical Activity of the Heart).
mhtml:mk:@MSITStore:C:\Users\deag1\Desktop\Review of Medical Physiology - Ganon...
5/19/2012
You might also like
- 300 NPTE Questions and Answers PTMASUD PDFDocument921 pages300 NPTE Questions and Answers PTMASUD PDFManik Mishra71% (7)
- AP Integumentary SystemDocument1 pageAP Integumentary Systemfrancy2010No ratings yet
- Autonomic Dysreflexia in Spinal Cord Injury Overview, Pathophysiology, Causes of Autonomic DysreflexiaDocument14 pagesAutonomic Dysreflexia in Spinal Cord Injury Overview, Pathophysiology, Causes of Autonomic Dysreflexiajacque zidaneNo ratings yet
- PRIN PBL Week 11 Tutorial 1Document3 pagesPRIN PBL Week 11 Tutorial 1jonx225No ratings yet
- Hipotensi PDFDocument6 pagesHipotensi PDFimahNo ratings yet
- Cardiovascular and Autonomic Influences On Blood Pressure: John E. Jones,, Aruna R. Natarajan,,, and Pedro A. JoseDocument23 pagesCardiovascular and Autonomic Influences On Blood Pressure: John E. Jones,, Aruna R. Natarajan,,, and Pedro A. JoseLulu LuwiiNo ratings yet
- Control of Blood Flow: After Reading This Chapter You Should Be Able ToDocument12 pagesControl of Blood Flow: After Reading This Chapter You Should Be Able ToDrbee10No ratings yet
- PR ThoraksDocument19 pagesPR ThoraksKevin KarimNo ratings yet
- Shock and Circulatory FailureDocument8 pagesShock and Circulatory FailureOktaviana Sari DewiNo ratings yet
- داتا حيداشر محاضرة فسيولوجىDocument6 pagesداتا حيداشر محاضرة فسيولوجىMohaned MokhtarNo ratings yet
- Pathophysiology of Myocardial InfarctionDocument4 pagesPathophysiology of Myocardial InfarctionYhr YhNo ratings yet
- SMW 09765Document10 pagesSMW 09765Erwan HermansyahNo ratings yet
- Pulsus Paradoxus - Wikip PDFDocument4 pagesPulsus Paradoxus - Wikip PDFAniket MittalNo ratings yet
- Pathophysiology of Ischemic Stroke - UpToDateDocument11 pagesPathophysiology of Ischemic Stroke - UpToDateKarla AldamaNo ratings yet
- Controlled Hypotensive AnesthesiaDocument24 pagesControlled Hypotensive AnesthesiaSuresh Kumar100% (1)
- Pathophysiology / Pharmacology: Cardiac PhysiologyDocument6 pagesPathophysiology / Pharmacology: Cardiac Physiologyjazzdoc007No ratings yet
- Shock: Pathophysiology, Diagnosis, Treatment, and Physiologic Response To TraumaDocument12 pagesShock: Pathophysiology, Diagnosis, Treatment, and Physiologic Response To TraumaValentinaJiménezNo ratings yet
- II-A ShockDocument5 pagesII-A ShockMuhammad075No ratings yet
- Blood PressureDocument8 pagesBlood PressureUmair RaoNo ratings yet
- Case 2 SlosDocument7 pagesCase 2 SlosNamarNo ratings yet
- Pulse PressureDocument7 pagesPulse PressureChrisNo ratings yet
- H FDocument23 pagesH FSaihmingliani SailoNo ratings yet
- CH27 FinalDocument8 pagesCH27 FinalDiogoBeirãoNo ratings yet
- Mechanisms, Causes, and Evaluation of Orthostatic Hypotension - UpToDateDocument20 pagesMechanisms, Causes, and Evaluation of Orthostatic Hypotension - UpToDateCipriano Di MauroNo ratings yet
- In The Name of Allah, The Most Beneficent, The Most MercifulDocument40 pagesIn The Name of Allah, The Most Beneficent, The Most MercifulISMAILNo ratings yet
- Wiki Ventricular RemodelingDocument3 pagesWiki Ventricular Remodelingdgina8800No ratings yet
- SHOCKDocument5 pagesSHOCKchidiebubesylviaokaforNo ratings yet
- Clinmed 21 3 E275Document8 pagesClinmed 21 3 E275Carlos CoronaNo ratings yet
- Haemodynamic Changes in Trauma: Editor's Key PointsDocument10 pagesHaemodynamic Changes in Trauma: Editor's Key PointsAlondra Lucero MejíaNo ratings yet
- Signs and SymptomsDocument16 pagesSigns and SymptomsRose AnnNo ratings yet
- Controlled HypotensionDocument21 pagesControlled HypotensionChristian YonathanNo ratings yet
- Hypovolemic ShockDocument10 pagesHypovolemic ShockUsran Ali BubinNo ratings yet
- Division 3: Trauma EmergenciesDocument125 pagesDivision 3: Trauma EmergenciesGaoudam NatarajanNo ratings yet
- Hypotension: Sandeep Sharma Priyanka T. BhattacharyaDocument10 pagesHypotension: Sandeep Sharma Priyanka T. Bhattacharyaمحمود محمدNo ratings yet
- Orthostatic Hypotension in Older AdultsFrom EverandOrthostatic Hypotension in Older AdultsAhmet Turan IsikNo ratings yet
- Cardiovascular Changes in CardiogenicDocument4 pagesCardiovascular Changes in CardiogenicBaso AgusofyangNo ratings yet
- CV PathoDocument32 pagesCV PathoSaif AliNo ratings yet
- Pathophysiology of Congestive Heart Failure NarrativeDocument4 pagesPathophysiology of Congestive Heart Failure NarrativeAlfred BucabucaNo ratings yet
- Dirk L. Brutsaert 1993-1Document8 pagesDirk L. Brutsaert 1993-1CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- HipotensiDocument12 pagesHipotensiAfdhalia Khairunnisa SyammarhanNo ratings yet
- Disreflexia AtonomicaDocument5 pagesDisreflexia AtonomicaNicolás Andrés MontanerNo ratings yet
- Compartment SyndromeDocument14 pagesCompartment SyndromedokteraanNo ratings yet
- TCHP Shock Series Part 2Document2 pagesTCHP Shock Series Part 2ikeernawatiNo ratings yet
- Shock - Critical Care Medicine - MSD Manual Professional EditionDocument8 pagesShock - Critical Care Medicine - MSD Manual Professional EditionSughosh MitraNo ratings yet
- Myocardial Infarction "Heart Attacks"Document16 pagesMyocardial Infarction "Heart Attacks"Camzii Borland100% (1)
- Cardiogenic Shock in Children: March 2012Document9 pagesCardiogenic Shock in Children: March 2012Quang TinNo ratings yet
- Shock: Shock Can Refer To A Range of Related Medical Conditions in Which The Victim's Heart, Lungs andDocument16 pagesShock: Shock Can Refer To A Range of Related Medical Conditions in Which The Victim's Heart, Lungs andLucreatia RynjahNo ratings yet
- The Normal Physiology of The Heart: Vikkineshwaran Siva SubramaniamDocument4 pagesThe Normal Physiology of The Heart: Vikkineshwaran Siva SubramaniamSivamala MalaNo ratings yet
- Increased ICPDocument7 pagesIncreased ICPK-La BreanneNo ratings yet
- Hypertensive Crisis PathoDocument4 pagesHypertensive Crisis PathoJanelle Dela CruzNo ratings yet
- Blood Pressure RegulationDocument3 pagesBlood Pressure RegulationiMaibelle BelleNo ratings yet
- Fisiopatología Shock 1980Document12 pagesFisiopatología Shock 1980Alejo ZubietaNo ratings yet
- Pathogenesis of The Raynaud PhenomenonDocument8 pagesPathogenesis of The Raynaud PhenomenonLuisAngelGuevaraRodriguezNo ratings yet
- Smith Intracranial HypertensionDocument55 pagesSmith Intracranial HypertensionElena-Dana OpreaNo ratings yet
- Cardiovascular Dysfunction in Spinal Cord DisordersDocument12 pagesCardiovascular Dysfunction in Spinal Cord DisordersGerardo SilvaNo ratings yet
- Peer Review Process: Author: Section Editor: Deputy EditorDocument14 pagesPeer Review Process: Author: Section Editor: Deputy EditorLuis Enrique Caceres AlavrezNo ratings yet
- Icu BookDocument1,054 pagesIcu BookqsychoNo ratings yet
- Askep Stroke NewDocument46 pagesAskep Stroke NewArkan RadityaNo ratings yet
- Project Injectable Hydrogels As Recent Advances in Treatment of Myocardial InfarctionDocument16 pagesProject Injectable Hydrogels As Recent Advances in Treatment of Myocardial Infarctionvarshankpathak2001No ratings yet
- Diastolic Dysfunction in Heart Failure Review LEEERRRDocument18 pagesDiastolic Dysfunction in Heart Failure Review LEEERRRchris chavezNo ratings yet
- CVS Pathophysiology of ShockDocument11 pagesCVS Pathophysiology of ShockSherwan R Shal100% (4)
- Dengue Guideline DengueDocument33 pagesDengue Guideline DenguedrkkdbNo ratings yet
- 3.3 Pathophysiology of Plasma LeakDocument1 page3.3 Pathophysiology of Plasma LeakM Adil AliNo ratings yet
- Dengue Guideline DengueDocument33 pagesDengue Guideline DenguedrkkdbNo ratings yet
- Guidelines For The Management of DF and DHF in AdultsDocument46 pagesGuidelines For The Management of DF and DHF in AdultsNanda SulistyaningrumNo ratings yet
- Guidelines On Management of DF and DHF in Children and AdolescentsDocument51 pagesGuidelines On Management of DF and DHF in Children and AdolescentsKhansa NalirNo ratings yet
- Dengue Mangement Charts and AlgorithmDocument15 pagesDengue Mangement Charts and AlgorithmM Adil AliNo ratings yet
- Research Article 08-09 Prof. Dr. Mehmood AyyazDocument5 pagesResearch Article 08-09 Prof. Dr. Mehmood AyyazM Adil AliNo ratings yet
- Minutes of Meetings Research Committee SIMS (2010-2011) .Document37 pagesMinutes of Meetings Research Committee SIMS (2010-2011) .M Adil AliNo ratings yet
- Acute and Chronic Wound HealingDocument114 pagesAcute and Chronic Wound HealingMARGARET BLANCHE NICOLASNo ratings yet
- Wound Healing, Tissue Repair, and FibrosisDocument28 pagesWound Healing, Tissue Repair, and FibrosisRibka Theodora100% (1)
- I-English Task D3 NursingDocument13 pagesI-English Task D3 NursingAdhwaNo ratings yet
- SkinDocument15 pagesSkinSnikitha SaiNo ratings yet
- Surgery, General, Wounds and Wound HealingDocument15 pagesSurgery, General, Wounds and Wound HealingRhazes78100% (1)
- Material Suture GUSTIDocument23 pagesMaterial Suture GUSTIChad CarverNo ratings yet
- Intro To Nursinhjcfnhgg - Exam 2 Concepts - Modules 5-8Document53 pagesIntro To Nursinhjcfnhgg - Exam 2 Concepts - Modules 5-8GovindSoniNo ratings yet
- Ozonated Oil in Wound Healing: What Has Already Been Proven?Document6 pagesOzonated Oil in Wound Healing: What Has Already Been Proven?Filipe GonçalvesNo ratings yet
- AntioxidantDocument6 pagesAntioxidantkumudhaveniNo ratings yet
- Safety Assesment of CalendulaDocument8 pagesSafety Assesment of CalendulaMahyumi ImpianNo ratings yet
- Basic Science and Sructure of Skin MCQsDocument92 pagesBasic Science and Sructure of Skin MCQsDr.Tawheed88% (16)
- Surgical Site Infection. Full NICE GuidelineDocument168 pagesSurgical Site Infection. Full NICE GuidelineIvan Villaverde Castillo100% (1)
- Effect of Astaxanthin On Cutaneous Wound Healing: Clinical, Cosmetic and Investigational Dermatology DoveDocument7 pagesEffect of Astaxanthin On Cutaneous Wound Healing: Clinical, Cosmetic and Investigational Dermatology DoveRaziel Alvarez RebolloNo ratings yet
- Biosensors and Bioelectronics: A 1 B 1 A BDocument14 pagesBiosensors and Bioelectronics: A 1 B 1 A BHozefa DhilaNo ratings yet
- Hyperbaric Oxygen TherapyDocument35 pagesHyperbaric Oxygen Therapybolinhaenf100% (1)
- 4d85 PDFDocument4 pages4d85 PDFSisca Dwi AgustinaNo ratings yet
- ABCDEFGHI Systematic Approach To Wound Assessment and ManagementDocument36 pagesABCDEFGHI Systematic Approach To Wound Assessment and ManagementsaerodinNo ratings yet
- Sodium Hyaluronate (Hyaluronic Acid) Promotes Migration of Human Corneal Epithelial Cells in VitroDocument2 pagesSodium Hyaluronate (Hyaluronic Acid) Promotes Migration of Human Corneal Epithelial Cells in VitroanamaghfirohNo ratings yet
- PreTest - Pathology Questions Multiple Choice Sample ExamDocument23 pagesPreTest - Pathology Questions Multiple Choice Sample ExamAdmin DutiesNo ratings yet
- Course of Lectures On Traumatic Injuries in Maxillo-Facial RegionDocument50 pagesCourse of Lectures On Traumatic Injuries in Maxillo-Facial RegionShany SchwarzwaldNo ratings yet
- Case Study WoundDocument4 pagesCase Study Wounddjokopri07100% (1)
- Management of Burns - NEJMDocument11 pagesManagement of Burns - NEJMOscar BedónNo ratings yet
- Inflammation and RepairDocument70 pagesInflammation and RepairmikeNo ratings yet
- Applied Anatomy and Physiology of CorneaDocument116 pagesApplied Anatomy and Physiology of CorneaJoubertnassif100% (1)
- Centella Asiatica - A Review of Its Medicinal Uses and Pharmacological EffectsDocument8 pagesCentella Asiatica - A Review of Its Medicinal Uses and Pharmacological Effectsjiva_shakti0No ratings yet
- Wound-TypesDocument1 pageWound-TypesJamie W.No ratings yet
- Cog Thread LiftDocument5 pagesCog Thread Liftemilly vidya71% (7)
- Wound Healing Activity of Niosomal Gel of Punicalagin From Peels of Punica GranatumDocument21 pagesWound Healing Activity of Niosomal Gel of Punicalagin From Peels of Punica GranatumSujith KuttanNo ratings yet