You might also like
- Circulatory System: A Tutorial Study GuideFrom EverandCirculatory System: A Tutorial Study GuideRating: 5 out of 5 stars5/5 (3)
- High Blood Pressure: Safe alternatives without drugsFrom EverandHigh Blood Pressure: Safe alternatives without drugsRating: 5 out of 5 stars5/5 (2)
- CH 03 HeartDocument20 pagesCH 03 HeartDarko SilipetarNo ratings yet
- Cardiac Cycle Made EasyDocument12 pagesCardiac Cycle Made EasyTA ĐặngNo ratings yet
- Systolic Cardiac Contraction) Times Heart Rate. So If You Increase Either One of So When Your Cardiac Output Goes Down, OurDocument5 pagesSystolic Cardiac Contraction) Times Heart Rate. So If You Increase Either One of So When Your Cardiac Output Goes Down, OurJohn RyNo ratings yet
- Cardiovascular System 2 Wan NajibDocument6 pagesCardiovascular System 2 Wan NajibAli Al-QudsiNo ratings yet
- Mitral Stenosis Made EasyDocument13 pagesMitral Stenosis Made EasyTuan Ahamed CassimNo ratings yet
- The Circulatory SystemDocument6 pagesThe Circulatory SystemAlberto ContadorNo ratings yet
- Heart Disease Book ChapsDocument70 pagesHeart Disease Book ChapsArpanpatelNo ratings yet
- The Circulatory System in MammalsDocument29 pagesThe Circulatory System in MammalsKeanna RaphaelNo ratings yet
- CSV4 Hemodynamics Continued-By Dr. KinnallyDocument11 pagesCSV4 Hemodynamics Continued-By Dr. KinnallyNYUCD17No ratings yet
- LO Dan WO Cardio Week 5Document60 pagesLO Dan WO Cardio Week 5Alan Dwi SetiawanNo ratings yet
- Cardiovascular System (Heart) : o o o o oDocument5 pagesCardiovascular System (Heart) : o o o o okayaldrNo ratings yet
- ATI Policy 2020Document12 pagesATI Policy 2020Abdullah AlsubhiNo ratings yet
- Cardiac Cycle ExplainedDocument5 pagesCardiac Cycle ExplainedCai Peng FeiNo ratings yet
- Cardiovascular SystemDocument6 pagesCardiovascular Systemtasneem8No ratings yet
- Coordinated Cycles of Heart Contraction Drive Double Circulate in MammalsDocument5 pagesCoordinated Cycles of Heart Contraction Drive Double Circulate in MammalsMayar HasanNo ratings yet
- The Circulatory System Group 2Document17 pagesThe Circulatory System Group 2sanique peterkinNo ratings yet
- LP-2 The HeartDocument6 pagesLP-2 The HeartDavidNo ratings yet
- Lesson 4 Cardiac CycleDocument24 pagesLesson 4 Cardiac CycleTristan PereyNo ratings yet
- How Does Heart Pump Blood:: Unit 1: Circulator SystemDocument32 pagesHow Does Heart Pump Blood:: Unit 1: Circulator SystemĐức PhạmNo ratings yet
- Heart and Circulatory SystemDocument5 pagesHeart and Circulatory SystemBryent GawNo ratings yet
- Anatomy of Heart - RyanDocument5 pagesAnatomy of Heart - Ryandrowned_clarkeNo ratings yet
- Anatomy of Heart - RyanDocument5 pagesAnatomy of Heart - Ryandrowned_clarkeNo ratings yet
- Cardiac CycleDocument2 pagesCardiac CycleAkil BabujiNo ratings yet
- Cardiac CycleDocument2 pagesCardiac CycleAkil BabujiNo ratings yet
- Cardiac CycleDocument2 pagesCardiac CycleAkil BabujiNo ratings yet
- Circulatory System of HumanDocument4 pagesCirculatory System of HumanLaraibNo ratings yet
- Anatomy of Heart - RyanDocument5 pagesAnatomy of Heart - Ryandrowned_clarkeNo ratings yet
- Hoppensteadt and Peskin - Chapter 1 - Student VersionDocument30 pagesHoppensteadt and Peskin - Chapter 1 - Student VersionchristiansassoNo ratings yet
- Acland's DVD Atlas of Human AnatomyDocument41 pagesAcland's DVD Atlas of Human AnatomyRaúl Flores RodríguezNo ratings yet
- Vital Sign: Blood Pressure and Its AlterationsDocument55 pagesVital Sign: Blood Pressure and Its Alterationsbemina jaNo ratings yet
- Exam For Self-GradingDocument11 pagesExam For Self-Gradingtayma 123No ratings yet
- The Cardiovascular System: Heart, Blood Vessels, BloodDocument9 pagesThe Cardiovascular System: Heart, Blood Vessels, BloodKrishnendu WorkNo ratings yet
- Circulatory System: Project ReportDocument11 pagesCirculatory System: Project ReportrajivpoplaiNo ratings yet
- Structure and Function of The HeartDocument5 pagesStructure and Function of The HeartThereseNo ratings yet
- Cardiogenic Shock NCLEX Review QuizDocument6 pagesCardiogenic Shock NCLEX Review QuizRegie Marie EvangelistaNo ratings yet
- The Circulatory SystemDocument10 pagesThe Circulatory SystemRezki RasyakNo ratings yet
- Circulation and Cardiovascular SystemDocument12 pagesCirculation and Cardiovascular SystemSatria MandalaNo ratings yet
- Ow Does The Heart WorkDocument2 pagesOw Does The Heart WorkMichaelben MichaelbenNo ratings yet
- Heart Dissection KEYDocument4 pagesHeart Dissection KEYAbiyad AhmedNo ratings yet
- The Heart Is A Muscle: BloodDocument8 pagesThe Heart Is A Muscle: BloodJhoewil QuintuaNo ratings yet
- Clinical PaperDocument18 pagesClinical Paperapi-356406300No ratings yet
- CAPEc 06Document30 pagesCAPEc 06Isheba Warren83% (6)
- The Circulatory System IsDocument4 pagesThe Circulatory System IsKieth ObaobNo ratings yet
- Jantung PDFDocument1 pageJantung PDFKarensa JanetNo ratings yet
- The Mammalian HeartDocument14 pagesThe Mammalian HeartAkili ArmaniNo ratings yet
- Anatomy For Beginners 2 - CirculationDocument18 pagesAnatomy For Beginners 2 - CirculationDefy R PradentyNo ratings yet
- Heart PathophysiologyDocument20 pagesHeart PathophysiologyDoctorDrapion100% (2)
- Cardio 1Document4 pagesCardio 1Liam Jacque LapuzNo ratings yet
- CVS McqsDocument5 pagesCVS McqsNishanthy PirabakarNo ratings yet
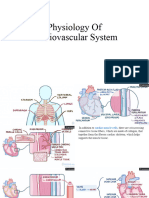
- Physiology of Cardiovascular SystemDocument19 pagesPhysiology of Cardiovascular SystemDavid JishkarianiNo ratings yet
- Cardiovascular Physiology - Dra. ValerioDocument16 pagesCardiovascular Physiology - Dra. ValerioAlexandra Duque-David100% (2)
- Heart MattersDocument7 pagesHeart MattersAbhishek SharmaNo ratings yet
- First Question: Student's Name: Adel Sulaiman SectionDocument5 pagesFirst Question: Student's Name: Adel Sulaiman SectionDental LecturesMMQNo ratings yet
- Circulatory System of MammalsDocument10 pagesCirculatory System of Mammalsben-jNo ratings yet
- Cardiovascular SystemDocument32 pagesCardiovascular SystemAugustus Alejandro ZenitNo ratings yet
- The Cardiovascular System: Arteries VeinsDocument27 pagesThe Cardiovascular System: Arteries VeinsMark Anthony DiegoNo ratings yet
- Human Circulatory System: The HeartDocument8 pagesHuman Circulatory System: The HeartRocheal WhittinghamNo ratings yet
- Med II-LE1-1.03 Arrhythmia NotesDocument14 pagesMed II-LE1-1.03 Arrhythmia NotesAbigael SantosNo ratings yet
- CVS - Charts & DiagramsDocument20 pagesCVS - Charts & DiagramsMamathaNo ratings yet
- Procedure in Assessing Blood PressureDocument4 pagesProcedure in Assessing Blood PressurecrrfrncNo ratings yet
- 13 Calibration WassertheurerDocument7 pages13 Calibration WassertheurerYasmine AbbaouiNo ratings yet
- Dr. Liliek, Sp. J - Cardiac ArrestDocument25 pagesDr. Liliek, Sp. J - Cardiac Arrestdhika2496No ratings yet
- Runninghead: Hypertension 1Document7 pagesRunninghead: Hypertension 1zakeyNo ratings yet
- SVT and DengueDocument4 pagesSVT and Denguefrengki prasNo ratings yet
- 1642 1645Document4 pages1642 1645Injit P. RianiNo ratings yet
- Atrial FibrillationDocument50 pagesAtrial Fibrillationvarun_swmNo ratings yet
- Ak Ku MulatorDocument20 pagesAk Ku MulatorNazrey MashudiNo ratings yet
- ECG Interpretation Cheat SheetDocument1 pageECG Interpretation Cheat Sheethirsi20051879% (24)
- Dysrhythmia Recognition Pocket Reference Card PDFDocument14 pagesDysrhythmia Recognition Pocket Reference Card PDFjenn1722100% (2)
- Perioperative ArrhythmiaDocument66 pagesPerioperative ArrhythmiaVithal DhulkhedNo ratings yet
- DR K Chan - Ecg For SVT Made EasyDocument66 pagesDR K Chan - Ecg For SVT Made Easyapi-346486620No ratings yet
- Atrial FibrillationDocument1 pageAtrial FibrillationRizia Emery SwedberghNo ratings yet
- Cardiac Cycle (Page Print 1-2)Document2 pagesCardiac Cycle (Page Print 1-2)hihariv794No ratings yet
- Drug Study DopamineDocument1 pageDrug Study Dopaminejulesubayubay542880% (5)
- Balon Contrapulsacion Autocat 2 WaveDocument32 pagesBalon Contrapulsacion Autocat 2 WaveCarito HernandezNo ratings yet
- Cardiology Dr. Payawal UltimateDocument9 pagesCardiology Dr. Payawal UltimateSven OrdanzaNo ratings yet
- NCLEX Cardiovascular Exam 2020 - Questions and AnswersDocument74 pagesNCLEX Cardiovascular Exam 2020 - Questions and AnswersNeoGellin83% (6)
- ACLS (Notes) (Printable)Document2 pagesACLS (Notes) (Printable)mike_germain1172No ratings yet
- Data Alkes KalibrasiDocument41 pagesData Alkes Kalibrasianisa13No ratings yet
- Heart Sound AnalysisDocument41 pagesHeart Sound AnalysisSoham RoyNo ratings yet
- Shock: Classification, Pathophysiology, and Approach To ManagementDocument45 pagesShock: Classification, Pathophysiology, and Approach To ManagementClaudia IsabelNo ratings yet
- (SVR) Measures Systemic Resistance and Reflects Afterload of Left Ventricle Average Perfusion of A Cardiac CycleDocument1 page(SVR) Measures Systemic Resistance and Reflects Afterload of Left Ventricle Average Perfusion of A Cardiac Cyclesarah_stover_1100% (4)
- ACLS Rhythms For The ACLS Algorithms: AppendixDocument32 pagesACLS Rhythms For The ACLS Algorithms: Appendixyan_ricci19100% (4)
- DefibrillatorDocument44 pagesDefibrillatorDipika JangpangiNo ratings yet
- ECG For BeginnersDocument61 pagesECG For Beginnersblndffl100% (2)
- ECG InterpretationDocument5 pagesECG InterpretationRichelle Dianne Ramos-Giang100% (3)
- Silent Ischemia and Ischemic Heart Disease - American Heart AssociationDocument4 pagesSilent Ischemia and Ischemic Heart Disease - American Heart AssociationKyaw SithuNo ratings yet