You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Arthritis E-Book DF PDFDocument14 pagesArthritis E-Book DF PDFManuel Anthony Lopez0% (1)
- Case Taking ProformaDocument7 pagesCase Taking ProformaDr Dushyant Kamal Dhari50% (2)
- Tear and Pterygium A Clinicopathological Study of Conjunctiva For Tear Film Anomaly in PterygiumDocument7 pagesTear and Pterygium A Clinicopathological Study of Conjunctiva For Tear Film Anomaly in PterygiumShofi Dhia AiniNo ratings yet
- Headache When To WorryDocument9 pagesHeadache When To Worryezra_putriNo ratings yet
- Clinico-Microbiological Spectrum of Hemodialysis Catheter-Related Blood Stream Infections: A Concise ReviewDocument7 pagesClinico-Microbiological Spectrum of Hemodialysis Catheter-Related Blood Stream Infections: A Concise ReviewIJAR JOURNALNo ratings yet
- NearfatalasthmaDocument8 pagesNearfatalasthmaHeath HensleyNo ratings yet
- Natural Medicine IODINE by Sue Visser.4810627Document3 pagesNatural Medicine IODINE by Sue Visser.4810627relativelabs2075No ratings yet
- Breastfeeding QuestionnaireDocument2 pagesBreastfeeding QuestionnaireDr Puteri Nur Sabrina Binti Mohd HanapiNo ratings yet
- Wing 1981 AspergerDocument15 pagesWing 1981 Asperger__aguNo ratings yet
- This Content Downloaded From 103.251.182.254 On Sat, 18 Jan 2020 04:52:17 UTCDocument9 pagesThis Content Downloaded From 103.251.182.254 On Sat, 18 Jan 2020 04:52:17 UTCsinnanancyNo ratings yet
- Nutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsDocument15 pagesNutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsIOSRjournalNo ratings yet
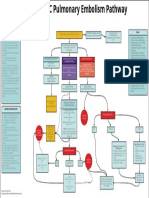
- EMCrit Lae Pulmonary FlowDocument1 pageEMCrit Lae Pulmonary FlowhmsptrNo ratings yet
- Foods and Purine ContentsDocument7 pagesFoods and Purine ContentsIndah ApsariNo ratings yet
- Cognosco, Brain Care Centre Newsletter: Summer 2013 IssueDocument28 pagesCognosco, Brain Care Centre Newsletter: Summer 2013 IssueBrain Care CentreNo ratings yet
- Physiology Study Guide CH 7 Nervous System Neurons KeyDocument4 pagesPhysiology Study Guide CH 7 Nervous System Neurons KeyJamie SamuelNo ratings yet
- How To Help Poor Countries: Nancy Birdsall, Dani Rodrik, and Arvind SubramanianDocument17 pagesHow To Help Poor Countries: Nancy Birdsall, Dani Rodrik, and Arvind SubramanianMarcus MonocayNo ratings yet
- Long Term Follow Up After Admin Human GT Products - Jan - 2020Document37 pagesLong Term Follow Up After Admin Human GT Products - Jan - 2020DNo ratings yet
- TPNDocument69 pagesTPNMylz MendozaNo ratings yet
- Chapter 39: Plant Responses To Internal and External SignalsDocument9 pagesChapter 39: Plant Responses To Internal and External SignalsdarthNo ratings yet
- Peritoneal DialysisDocument3 pagesPeritoneal DialysisSumit YadavNo ratings yet
- PERIDA EMMALYN T. - BSci103-Lesson 4.2-Learning TaskDocument5 pagesPERIDA EMMALYN T. - BSci103-Lesson 4.2-Learning TaskEmmalyn PeridaNo ratings yet
- Export Act 1963Document27 pagesExport Act 1963Anonymous OPix6Tyk5INo ratings yet
- QUES2-1 Stir Not The World's DoomDocument49 pagesQUES2-1 Stir Not The World's DoomNicholas LouieNo ratings yet
- Your Body Believes Every Word Y - Barbara Hoberman LevineDocument380 pagesYour Body Believes Every Word Y - Barbara Hoberman LevineRoryBradshawNo ratings yet
- Spine Magnetic Resonance Image Segmentation Using Deep Learning TechniquesDocument6 pagesSpine Magnetic Resonance Image Segmentation Using Deep Learning TechniquesSandeep VermaNo ratings yet
- Lapsus Dr. DodyDocument36 pagesLapsus Dr. DodyPriscilla Christina NatanNo ratings yet
- Diabetes Transformation Summit 2022 Day 3Document5 pagesDiabetes Transformation Summit 2022 Day 3Paul Ioan PopescuNo ratings yet
- En Abbott Realtime Sars-Cov-2: For Use Under An Emergency Use Authorization (Eua) OnlyDocument12 pagesEn Abbott Realtime Sars-Cov-2: For Use Under An Emergency Use Authorization (Eua) OnlyDevi OktaviannyNo ratings yet
- Struggle and Survival of Native Americans: A Study in Selected Poems by Simon J. OrtizDocument15 pagesStruggle and Survival of Native Americans: A Study in Selected Poems by Simon J. OrtizCycilian ArmandoNo ratings yet
- Evolution in Teddy Grahams MTDocument1 pageEvolution in Teddy Grahams MTapi-302703920No ratings yet