Professional Documents
Culture Documents
DMD Seminar SHPTSK
Uploaded by
luongthangOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
DMD Seminar SHPTSK
Uploaded by
luongthangCopyright:
Available Formats
Allllu. Rev. Gellet. 1988.
22:601-29
Copyright 1988 by Annual Reviews Inc. All rights reserved
LP1Lb L L\LPP
N\bL\LPK LXb1KLX
Ronald G. Worton
Department of Genetics and Research Institute, The Hospital for Sick Children, and
the Departments of Medical Genetics and Biophysics, University of Toronto, 555
University Avenue, Toronto, Ontario M5G IX8 Canada
Margaret W. Thompson
Departments of Genetics and Pediatrics and Research Institute, The Hospital for Sick
Children, and the Departments of Medical Genetics and Pediatrics, University of
Toronto, 555 University Avenue, Toronto, Ontario M5G IX8 Canada
CONTENTS
INTRODUCTION. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 602
CLASSICAL GENETICS OF DUCHENNE AND BECKER MUSCULAR
DySTROPHy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 602
MOLECULAR GENETICS OF DMD AND BMD .. ......... . . .. ... . . . .. ................ . . .. . 603
Mapping the DMD Gene to Chromosome Band Xp21 .... . . . . ... ................ . . . . . .... 63
Cloning of DNA Segments from the DMD Locus............. . ................... . . ....... 606
I solation of Expressed Sequences from the DMD Gene. . .. . . ...... .............. .. . .. .... 609
Cartography of the DMD Gene..... ... ................... 61 2
MUTATION ANALYSIS AND CLINICAL APPLICATIONS . . . . ............... . ... . . ..... 61 2
Nature of Mutations i n the DMD Gene ................... . ... . . . . .... . . . . . . . . . . . . . . ....... . . 61 2
Carrier Identification and Prenatal Diagnosis......... . .. ... . . . . . .................. . . . ..... 61 4
DYSTROPHIN, THE PROTEIN PRODUCT OF THE DMD GENE ........... . .. . ....... 61 6
Expression of the DMD Gene... . . . . .. . ...... ........... . .... .. . . . . ................. . . . . ....... 61 7
Dystrophin Structure Deduced from cDNA Sequence. ... ... . . . . . ................ . . . . ...... 61 7
Localization of Dystrophin in the Muscle Cell............... . . . . .................. .. ....... 61 8
Pathogenesis of the Disease ...... . . . . .... . . ... . . .......... ... ... "" ................... . . . . . .. 61 9
Animal Models... . ........... .. ............. . . ... . ..... . . ................ . . . . . ................ . .. . 620
APPLICATIONS OF REVERSE GENETICS TO OTHER DISEASES. . . . . . . . . . . . . . . . . . . . 621
Contiguous Gene Syndromes.. . .. ........... .. . . . . . . . .... . ................ . . . . ................ . 621
X/Autosome Translocations ....... .. . ... ... .. .. .... .. ....... . ........ . .... .. . . . ...... .......... 622
CONCLUSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 622
601
0066-4197/88/1215-0601 $02.00
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
Quick links to online content
Further
ANNUAL
REVIEWS
602 WORTON & THOMPSON
INTRODUCTION
Duchenne muscular dystrophy (DMD) is a lethal X-linked genetic disease that
for many years was one of the most perplexing and frustrating disorders in
clinical genetics. Until the advent of molecular genetic approaches, the nature
of the primary defect remained elusive. All attempts to detect an altered
protein in muscle tissue, cultured muscle cells, or other tissues from patients
had yielded negative results. Attempts to determine the basic biochemical or
physiological defect were frustrated by the difficulty of distinguishing the
primary defect from the numerous secondary manifestations of the disease
(38, 102, 109, 131, 132). The same difficulty also handicapped attempts to
identify carriers and carry out accurate prenatal diagnosis in Duchenne fami
lies (55).
Prospects for understanding the disease changed dramatically about 1983,
when the gene responsible for DMD was mapped to a specific region of the X
chromosome, and strategies were devised to clone it by reverse genetics from
knowledge of its map position, bypassing the need to know anything about the
protein product. In the last five years, isolation of genomic sequences from
the site of the gene has led to isolation of the complete expressed gene
(cDNA) and identification of dystrophin, the gene product of the normal allele
(64). A complete understanding of the disorder cannot be far away.
CLASSICAL GENETICS OF DUCHENNE AND BECKER
MUSCULAR DYSTROPHY
The clinical and genetic aspects of DMD and the milder Becker muscular
dystrophy (BMD) have been well reviewed recently (38, 39, 53) and are
summarized only briefly here.
Patients with DMD present with muscle weakness at the age of 2 to 5 years
lose the ability to walk at about the age of II years and do not usually survive
beyond the early twenties. A consistent finding is the grossly elevated level of
serum creatine kinase (CK), especially in the preclinical and early clinical
stages of the disease. CK is also elevated, though to a lesser degree, in the
serum of about two thirds of carriers, providing a useful though not definitive
carrier test (38, 39).
BMD resembles DMD, but until recently it had been considered a separate
entity because of its later onset, more benign course, and longer survival.
Generally patients with BMD are defined as those who are still ambulant at
the age of 16 years. In a minority of cases, the disease is intermediate in
severity between DMD and BMD. BMD also resembles autosomal recessive
limb-girdle muscular dystrophy and may be confused with it if there is no
family history (38, 53). BMD and DMD are now known to be caused by
mutations in the same gene, designated DMD.
Because the DMD gene is X-linked and subject to random inactivation,
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 603
expression in a proportion of carriers is to be expected. According to one
estimate (38), about 8% of carriers have some clinical manifestation of
myopathy. The disorder is also regularly expressed in female carriers with a
45, X karyotype in some or all cells (reviewed in 7). As discussed below, a
number of manifesting females with X/autosome translocations have been of
special significance for our understanding of the disease.
The expression of DMD/BMD in monozygotic female twin carriers has
been of special interest since Gomez and colleagues reported severe clinical
manifestations in one carrier but not in her monozygotic twin sister (47).
Several similar cases have since been reported (reviewed in 107). Uneven
X-inactivation can bring about marked discrepancy in clinical expression of
an X-linked trait between members of an identical twin pair, and studies of
one pair of DMD carriers have suggested that the twin sisters had preferential
ly inactivated different X chromosomes (15). The possible embryonic
relationship between the twinning event and the development of different
X-inactivation patterns in the co-twins remains unclear.
Most estimates of the incidence of DMD are in the range of 2.7 to 2.9 x
10-4 (I in 3300-1 in 3700) male births, with little if any ethnic variation (74,
101, 103, 127). The mutation rate of close to I x 10-4 is an order of
magnitude higher than most other known mutation rates. The extremely large
size of the target for mutational events (2000 kb) plus mutational hotspots in
the gene appear to account for this high rate (see below).
The question of a possible sex difference in mutation rate is of more than
theoretical importance, since genetic counseling for DMD assumes equal
mutation rates in male and female. In accordance with the Haldane rule, this
assumption allows the calculation that one third of all cases should result from
new mutation in the maternal gamete, one third by inheritance of the DMD
gene from a carrier mother who is herself a new mutant, and one third by
inheritance of a DMD gene present in an earlier generation. The results of
segregation analysis in several large studies (25, 74, 101, Il l , 127, 134) are
in most but not all cases consistent with this expectation.
The relative proportion of mutations at the locus that result in BMD rather
than DMD is small. Calculation by Haldane's formula with fitness estimated
as 0.70 (37) reveals that only 10% of Becker patients are new mutants. BMD
is reported to account for 11-17% of mutations at the locus (103), with an
incidence of 3.4-5. 5 x 10-5. The corresponding mutation rate would be
3.4-5.5 x 1O-1, about 3-5% of that for DMD.
MOLECULAR GENETICS OF DMD AND BMD
Mapping the Gene to Chromosome Band Xp21
The first indication that the gene responsible for DMD and BMD is in band
Xp2l in the X-chromosome short arm came from rare females with the
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
60 WORTON & THOMPSON
Duchenne or Becker phenotype. In the late 1 970s and early 1 980s, several
affected girls were described (16, 36, 73, 91, 1 22, 137), each of whom had a
de novo X autosome translocation with a breakpoint in band Xp21 (Figure
lA). The consistent involvement of band Xp21 suggested that a gene at this
site might have been disrupted by the translocation, while preferential in
activation of the unrearranged X chromosome was presumed to silence the
coresponding normal allele, leading to the phenotypic expression of an
X-linked disease in a "carrier" female. Several further cases (Figure l A) have
been ascertained, and the exchange points have always involved band Xp21
(reviewed in 8, 1 0, 38, 1 32). In three cases, RLP markers (77) or cytogene
tic polymorphisms (46, 108a) have demonstrated pateral origin of the
translocation.
High resolution banding analysis of several of the translocations revealed
heterogeneity of translocation exchange points within Xp2 1 , with some ex
changes in Xp21 . 1 , most in Xp21 . 2, and a few at the centromeric edge of
Xp21. 3 (Figure lA) (8, 9, 1 0) . Since band Xp2 1 . 2 spans 2-3 million bp of
p21
p21.3
p21.1
t(X;3)
tf"
t(X;2)
t(X;5)
-- t(X 6)
t(X;9)
t(X;5)
t(X;11)
t(X;21)
_..
..
..
]- ...
.
.
}MD
_
Kl00
J- ..
_..
.
... ..
Llnkag
Map
Figure 1 Schematic of the three lines of evidence mapping the DMD gene to band Xp21.
A. Chromosomal localization of translocation exchange points in females with OMO or BMO.
High resolution banding by Boyd & Buckle (8) revealed a heterogeneity of exchange points
between the upper edge of band Xp21.1 and the lower edge of band Xp21.3. a region spanning a
few million base pairs of DNA. The trans locations shown were originally described in references
4b. 5. 16,36, 70a, 73, 91, 104b, 107a, 122, and 137. Additional translocations not included in
the Boyd and Buckle study are found in references 104a, 108a, and 111 a.
B. Several anonymous probes and the OTe (orithine transcarbamylase) gene map to the short
arm of the X chromosome, as shown. These probes reveal RFPs that segregate with the DMD
and BMD phenotype in families. The estimated genetic distance between DMD and the markers
is shown on the right hand scale in cM. A more detailed review of the segregation data is found in
Goodfellow et al (48) and Worton & Burghes (132).
C. The deletion in patient BB is microscopically visible and confers a complex phenotype that
includes DMD, XK, eGD, RP, and mental retardation (44). See text for more detail and for
references to other deletion patients. DNA, this suggested that the DMD gene might be very large
or that some of
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 605
the exchange points might lie outside the gene and disrupt its activity through
an alteration of chromatin configuration that extended along the chromosome.
The molecular mapping of these exchange points relative to the DMD gene is
discussed in a later section.
The second line of evidence placing the DMD gene at Xp21 came from
family studies with DNA probes that detect restriction fragment length
polymorphism (RFLP) on the human X chromosome. The first two linked
markers for the DMD gene were the RFLPs detected by the probes RC8 (104)
and Ll . 28 (31 ) . The RC8 clone mapped to the distal third of the short a of
the X chromosome while Ll. 28 mapped to the proximal third (Figure I B). In
Duchenne families both polymorphic markers were found to segregate with
the DMD gene, but each displayed a recombination frequency of about 20%,
placing the two probes at a linkage distance of 20 cM from the DMD gene.
The two probes mapped about 40 cM apart, indicating that they must flank the
DMD gene, mapping the gene to the middle of the short a (31) .
Since these initial reports, many more Xp probes have been isolated,
mapped, and found to be linked to the DMD gene at distances from 10 to 20
cM (30, 48). Figure IB shows some of these probes and their estimated
l inkage distances from the DMD gene. Of note are the two closest random
probes, C7 on the telomeric side (34) and 754 on the centromeric side of the
gene (70).
In Becker families, the same probes revealed a segregation patter similar
to that for DMD, thereby mapping the responsible gene to band Xp21 and
providing the first indication that the severe Duchenne form and the milder
Becker form might be caused by mutations in the same gene (80).
The third line of evidence placing the DMD gene at Xp21 came from a
small set of patients with complex phenotypes including DMD, with one or
more of several X-linked phenotypes including glycerol kinase (GK) de
ficiency, adrenal hypoplasia (AHC), retinitis pigmentosa (RP), McLeod phe
notype (XK) , and chronic granulomatous disease (CGD) . A syndrome of
Duchenne dystrophy coupled with AHC, GK deficiency, and mental retarda
tion (MR) had been recognized in families with two or more afected males,
suggesting X-linked inheritance and the possibility that the phenotypes result
from the deletion of three or more contiguous genes (reviewed in 43).
Although patients with DMD and CGD or XK with CGD had been known
for some time, the first concrete evidence for a deletion of contiguous genes
came from study of BB, a patient with DMD, CGD, XK, and RP (4).
Cytogenetic analysis with high resolution chromosome banding revealed a
small but detectable deletion of part of bands Xp2 1 . 1 and Xp21. 2 (Figure
I C) . Verification that the deleted segment was not reinserted elsewhere in the
genome required study of the DNA directly. At the time, the random DNA
segment, 754, (Figure IB) had been shown to segregate at high frequency
with the DMD gene (70). Souther blot analysis of BB's DNA revealed no
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
606 WORTON & THOMPSON
hybridization signal with probe 754, dramatic proof that there was a deletion
of DNA from Xp21 without reinsertion elsewhere in the genome. Sub
sequently other patients, each with multiple X-linked disorders, were reex
amined by high resolution banding and tested for hybridization to 754 and
other Xp21 probes. This revealed a number of deletions and confirmed the
concept of complex phenotypes resulting from deletions of contiguous genes.
Several recent papers review the extent of the various deletions and clearly
demonstrate a most probable gene order of AHC, GK, DMD, XK, CGD, RP
in a telomere-to-centromere direction (3, 1 9, 21 , 27, 30a, 35, 43, 1 20). It is
noteworthy that two patients with isolated DMD have been described with
cytogenetically visible deletions extending from 754 into the DMD gene (52,
1 26) .
Thus, the combination of translocation exchange points, linkage analysis,
and contiguous gene deletions confirmed the mapping of DMD plus several
other disease loci to Xp21 and set the stage for the gene cloning strategies
described below.
Cloning of DNA Segments from the DMD Locus
The human X chromosome contains about 5% of the genome or 150,000 kb,
and the closest randomly isolated segments were about 10 cM from the DMD
gene, a physical distance estimated to be about 10,000 kb. The following
strategies were designed to enhance the chance of finding DNA sequences
from within the DMD gene.
One strategy was a clever but unfortunately unsuccessful attempt to clone
the gene by screening an X chromosome-specific genomic library against
cDNA l ibraries prepared from normal muscle mRNA, in a search for X
chromosome sequences expressed in muscle. The one candidate gene isolated
was an X-linked pseudogene of the glyceraldehyde-3-phosphate de
hydrogenase gene, which itself maps to chromosome 1 2 (4).
Two other strategies which were designed to take advantage of unique
patients with structural rearrangements at the site of the gene have been
successful in isolating genomic clones from within the gene.
The approach of Kunkel and his colleagues (86) depended on the isolation
of multiple clones from within a small region of the X chromosome known to
be deleted in BB, one of the patients with a complex phenotype (Figure IC).
The strategy is outlined in Figure 2A. DNA from an XXXXY male (to enrich
for X chromosome sequences) was cleaved with the restriction endonuclease
Mbo!. Sheared DNA from patient BB was added in large excess in a competi
tive hybridization reaction (the phenol enhanced reassociation technique
pERT) to compete selectively with all sequences except those from the
deleted segment. Following denaturation and reassociation, hybrid molecules
containing two sheared strands or those containing a sheared strand and an
MboI-digested strand would be refractory to cloning. The rare hybrid mole-
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 607
cules consisting of two MboI-digested fragments were compatible with clon
ing into a BamHl- cleaved vector and these molecules were enriched for
sequences from the region deleted in BB, since there was no competing
sheared DNA from this region (86, (8).
Following pERT reassociation, the renatured DNA was ligated to a BamHI
cleaved plasmid and the resulting library was tested clone by clone to identify
those clones that mapped within the BB deletion. Among a few hundred
pERT clones analyzed, eight failed to hybridize to a Souther blot of DNA
from BB and therefore mapped within the BB deletion (86, 98).
Each of these clones was then tested for hybridization to DNA from a series
of male DMD patients, on the assumption that some patients might have
deletions of all or a portion of the DMD gene and that any pERT clone that
failed to hybridize with the patient's DNA might map within or close to the
gene. Among the eight pERT clones from withing the BB deletion, one clone,
P. b!cloning
XXXXY
DNA
Mbol
M.M
+.+
MM
del.
DNA
shear
==
.
100
m
00hIu|0
tcntute
m
CLONE
. t (X ; 21 ) (p21 ; q12) translocation
"" :
p1 r
p1 -.
_ _
)
rDNA
X 21
der (X) der (21)
Figure 2 Schematic to illustrate the two successful cloning strategies.
A. The pERT cloning scheme is described in the text . The ends of the MboI-digested molecules
are indicated as M (double stranded) or m (single stranded). The ends of the sheared molecules
are unlabeled. Among the reassociated molecules, only the perfectly aligned MboI-digested
molecules are clonable, and these are enriched for sequences missing from the DNA of patient
BB.
B. The translocation junction cloning scheme is described in the text. The der(X) and der(21 )
chromosomes from the t(X;21) translocation patient , AH, were separated from other ribosomal
gene-bearing chromosomes by segregation in somatic cell hybrids, and ribosomal gene probes
were used to identify and clune a DNA fragment spanning the junction, XJ. The X-chromosome
side of the junction was expected to be derived from the DMD gene. The block of ribosomal
genes disrupted by the translocation is marked rONA. Only the short arms of the chromosomes
are shown.
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
608 WORTON & THOMPSON
pERT87, seemed to be the closest, since DNA from 5 of 57 DMD patients
lacked the pERT87 sequence (98).
The pERT87 sequence then became the startpoint for a bidirectional
chromosome walk along a normal X chromosome by the sequential isolation
of overlapping phage clones from an X-chromosome enriched library (86, 99,
100). Eventually, 220 kb of the X chromosome was isolated, and this DNA
segment was given the locus designation of DXS164. During the chromosome
walk several single copy segments were identified and the first three of these,
pERT87- 1 , 87-8, and 87- 1 5, were distributed to many laboratories around the
world for analysis of patient DNA. Twenty-five l aboratories contributed data
on deletions, and a total of 88 deletions were recorded in 1 346 patients
examined (85). In over half of these, the deletion extended through the entire
DXS164 region, but in some patients the deletion extended from within
DXS164 toward either the centromere or the telomere. Since these deletions
did not define a minimum region of overlap, it appeared that there must be
elements of the DMD gene on both sides of the DXS164 locus. However, one
patient had a 45 kb deletion from within the DXS164 locus, suggesting that an
important part of the gene must reside within this region. Two of the deletion
cases (85) and others reported subsequently (56, 57) were classified as BMD,
confirming that BMD and DMD are caused by allelic mutations (85). A
detailed map of the endpoints of many of these deletions is provided by
Monaco and colleagues (96) . The position and orientation of the pERT87
probes in the DXS164 locus is shown in Figure 3.
Since the DXS164 locus seemed by deletion analysis to be part of the DMD
gene, it was anticipated that pERT probes should invariably segregate with
the DMD gene in families. Some of the pERT87 probes were found to detect
RFLPs, and when these were used as markers in family studies, they segre
gated with the mutant gene in only 95% of meioses (4a, 40). The 5%
recombination rate was puzzling and indicated an average genetic distance of
5 eM between pERT87 probes and the mutation site, a result which has since
been demonstrated to be due to intragenic recombination and to misclassifica
tion of carriers with gonadal mosaicism (see below).
We retur later to a discussion of the DXS164 locus in connection with
isolation of expressed sequences.
The second successful approach leading to the DMD gene was that taken by
our group. The approach was dependent on the identification of a transloca
tion female with a rearrangement that placed the translocated segment from
her X chromosome adjacent to a block of tandemly repeated genes encoding
the 1 8S and 28S ribosomal RNA ( 122, 133) (Figure 2B). Ribosomal DNA
(rDNA) probes isolated in the laboratory of R. Schmickel were used to
identify and clone from the patient a segment of DNA that spanned the
translocation junction ( 1 08). This cloned segment was obtained from a
mouse-human somatic cell hybrid containing the der(X) (Figure 2B)
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 609
translocation chromosome ( 1 33). The hybrid cell line had been cultured for
many months to allow time for the loss of human acrocentric chromosomes,
which together carry 300-00 copies of the ribosomal genes, thereby simpli
fying the search for an X-rDNA junction fragment .
The junction clone designated XJI contained 620 bp of rDNA at one end,
and about 1 1 kb of X-chromosome sequences at the other. Chromosome
walking from XII along a normal X chromosome yielded about 1 20 kb of the
human X chromosome (the DXS206 locus) derived from both sides of the
junction site. Within the DXS20610cus three subclones, XJ l . l , 1 . 2, and 2. 3 ,
detected RFLPs that segregated in Duchenne families with the DMD muta
tions. Like pERT87, Xl probes showed approximately 5% recombination
between the probe site and the DMD mutations ( 1 1 9) and detected deletions in
about 6% of male patients ( 1 08) .
Figure 3 shows the relation between DXS206 and DXS164 on the short arm
of the X chromosome. Since the XJl clone came from the der(X) chromo
some (Figure 2B) carrying X chromosome sequences from the centromeric
side of the junction, it provided an orientation of the DXS206 locus with
respect to the centromere and telomere. The pERT87 probes were found to
hybridize with DNA from the somatic cell hybrid line carrying the der(21 )
translocation chromosome (Figure 2B) but not the der(X) chromosome, there
by mapping DXS164 on the telomeric side of DXS206 (85). Patients who had
deletions of DXS206 and the pERT 87-1 end of DXS164 provided the
orientation of DXS164 on the chromosome (56). Eventuall y, chromosome
walking closed the gap between DXS164 and DXS206, with 1 67 kb between
the original pERT87- 1 clone and the XJl clone at the t(X;21 ) junction. The
combined walks covered 340 kb of the X chromosome.
Before the isolation of cDNA clones, there was considerable uncertainty as
to whether the DXS164IDXS206 region was interal to the DMD gene. We, in
particular, were concered that the t(X;21 ) translocation might have involved
a submicroscopic deletion of several hundred kb that removed the DMD gene.
If this was the case, the XJ1 clone could have been derived from a sequence at
a considerable distance from the DMD gene on a normal chromosome. This
possibility was eliminated by the isolation and sequence analysis of the
t(X;2 1) translocation junction from both derivative chromosomes. Sequenc
ing revealed small deletions of about 20 bp from the rDNA complex on
chromosome 21 and about 70 bp from the X chromosome (6). The lack of a
major deletion reinforced the concept that the translocation had caused the
disease by disruption of a gene at the site of the translocation. Additional
evidence came from the finding of patients with deletions confined to the
DXS206 locus (56, 1 1 8).
Isolation of Expressed Sequences from the DMD Gene
Since the evidence was strong that the DXS164 and DXS20610ci were within
or very close to the DMD gene, the strategy to locate exons of the gene was to
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
61 0 WORTON & THOMPSON
Z1d
... g00m|C
g0D0 C|00S
1l3o!
C0Clg
11
S00u0C0
,^ ,,
,30
z5
\
.
\
.
i/
J6
V
E
R
.
L
X o 0
N
.
mul8l0q
S| 10S
L X.Z)
{X1|
l[X,d|
l(X:5)
l[X,4)
{X,11|
l(X;22)
_00!0l|0
..
188
t C0lOl|o
754 +
CX5.4
'
1{X1|
o XK
CGD
o
O
[
C
m I
H2b
0on
7
/ ' : i
W{X,1)
..
H
0xo 3
H. J-
47
n
00D2
l
1[X,b|
00n 1 U
[
{X,11|
L14 I0m0l0
(DXS1
4
2\
|
ma
.
0
o
l0
aS0S
1=00
Figure 3 Genomic map of the DMD gene. The section on the left shows the relation between
band Xp21 and the original pERT87 and XJ regions (DXSl6 and DXS206). These map within
the DMD gene and are flanked by the GK and AHC genes on the telomeric side and the XK. CGD.
RP, and aTC genes on the centromeric side. The anonymous probes C7 and 754 are described in
Figure I. Probe L (Kunkel et ai, 86a) is non-polymorphic and maps at least 1 5,000 kb from
DMD. Probe CX5.4 (69) maps proximal to DMD, probably between the aTC and 754 loci. On
this stick diagram, only the DXSl6 and DXS206 loci are drawn to the scale on the right-hand
side. The DMD gene is shown in the middle of the figure and is drawn to the right side. Beside the
gene is a schematic of the various cloned regions discussed in the text. The "jump" clones J-66,
JBir, J-MD, and J-47 were derived by isolation of deletion junction clones with pERT87 probes
and are therefore shown attached to the DXSl6 locus by a dashed line. pERT84 was an
independent clone derived from the original pERT screen and was later shown to map near the
first exon of the gene. The clones GMGXl l , P20, HIP25 , HH, and the "Heilig walk" are
discussed in the text. The DXS206 locus was expanded from its initial 120 kb size by cosmid
walking with cDNA clones as probes. It was extended through exons 3-7 in a continuous block.
Exons I and 2 lie on cosmids that have not as yet been linked to each other or to the DXS206
locus, so they are attached to the DXS206 locus by a dashed line. The cosmid clone containing
exon 1 also carries the promoter of the gene (81) and the ATG translocation start signal (82).
Many of these genomic clones have been mapped by PFGE or FlGE analysis onto specific Sf
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 611
test individual genomic subclones for hybridization with expressed sequences
(RNA or cDNA) from muscle and/or to test for sequences conserved across
species. Monaco et al ( 1 00) reported the first exons in the DXSl64 locus by
identifying a subclone, pERT87-25, that hybridized with monkey, bovine,
mouse, hamster and chicken DNA in a "zoo blot." The pERT87-25 clone
contained an exon-like sequence (open reading frame with appropriate 5' and
3' splice junctions) that was conserved precisely in mouse DNA, revealed a
message of -16 kb (later estimated at 14 kb) on Norther blot analysis of
muscle, and identified a l-kb cDNA clone from a fetal skeletal muscle eDNA
library. The cDNA clone contained 8 exons that mapped into the DXS164
locus over a span of 1 30 kb (Figure 3). Sequence analysis indicated an orientation
with tanscription in a centomere-to-telomere direction. Rescreening of the
cDNA library allowed isolation of overlapping cDNA clones correspnding
eventually to a complete representation of te 14 kb tanscript (82). The complete
set of cDNA clones hybridize with at least 60 different Hind il fragments on
genomic Souther blots, and since the cDNA contains few Hind il sites, most
fragments must contain one or more exons of the gene. The frst 33 exon
containing fagments mapped over a genomic distance of -10 kb, suggesting
that the total gene might be about 200 kb in size.
In our own laboratory an extensive search for conserved sequences within
the DXS206 locus initially failed to yield positive results, a consequence of
the fact that the DXS206 locus ( 1 20 kb at the time) contains an intron of 1 1 0
kb surrounding the t(X;21 ) translocation junction. Eventually, two subclones
from XJlO (XJl O. 2 XJlO.3), located about 55 kb on the telomeric side of the
t(X;2l ) junction (Figure 3), identified a 2-kb cDNA from an adult muscle
eDNA library ( 1 2) . This eDNA clone contained the first 1 6 exons at the 5'
end of the gene, with exons 1 -7 mapping on the der(X) chromosome and
exons 8-1 6 on the der(21) chromosome ( 12) , thus confirming that the t(X;21)
translocation had disrupted the gene to cause the disease. Several of the exons
on the 3' side mapped to the DXS164 locus and were identical with the first
set of exons identified by Monaco and colleagues ( l 00) . A linear map of all
<
fragments. The SfI map ( 1 21 ) is shown on the right side with fragment size (kb). The solid circles
represent sites that always cut with the enzyme while the open circles represent sites that fail to
cut in some molecules, perhaps due to methylation ( 1 21 ) . The mutation sites shown include
several translocation exchange points that have been mapped relative to genomic probes by Boyd
et al (9, 10), the edge of the BB deletion ( 44), and a deletion hotspot that is discussed in the text
and diagrammed on the cDNA map of Figure 4. Exons 1 020 lie in the DXSl64 locus, exons 8
and 9 in the original DXS206 locus. Exons 3-7 like in the DXS206 locus expanded by cosmid
walking. The distance between exons I and 2 and between 3 and 4 are unknown but are shown to
be large because exon 1 lies near pERT84 and van Ommen places pERT84 near the centromeric
end of the 720 kb SfI fragment ( 1 20). There are over 40 exons above the DXSl64 locus (82) that
have not as yet been accurately mapped and the 3' end of the gene is undetermined. The
minimum size of the gene appears to be about 2000 kb.
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
61 2 WORTON & THOMPSON
the exon-containing HindIII fragments is provided by Koenig and colleagues
(82). A more detailed map of the first 20 exons is nearing completion as the
cDNA probes have been used to extend the DXS206 locus by the isolation of
cosmid clones containing much of the 5 end of the gene (95) including the
promoter region (81) .
Cartography of the DMD Gene
With a gene of this size (Figure 3), conventional restriction mapping is
inadequate, but the newer techniques of pulsed field gel electophoresis
(PFGE) and field inversion gel electrophoresis (FIGE) have been ideal for
constructing long-range restriction maps of large DNA fragments ( 1 3, 1 4, 78,
1 20, 1 21 ) . For simplicity, only the SfiI sites are shown in Figure 3. The
restriction map is anchored to the DMD map by the SfH site in DXSl6 ( 1 3,
59, 1 21) . Several other genomic clones are depicted in Figure 3, and these
serve as useful landmarks on the genomic map. The "jump" clones J-47,
J-MD, J-Bir, and J-66 were all obtained using pERT87 probes to detect and
isolate aberrant restriction fragments that spanned the deletion junctions of
four patients whose deletions extended from DXS164 to the region of the
"jump" clone (96,99) . Each "jump" clone sequence formed the basis for short
chromosomal walks to isolate the genomic regions indicated. The clone
HIP25 (Figure 3) was isolated by Davies' group with a technique analogous to
pERT, but using high inorganic phosphate (HIP) to enhance the reassociation
(114) . The clone HHI was obtained by a chromosomal hop (HIP HOP) from
HIP25 (79) . A portion of the DXS164IDXS206 loci has also been isolated by
Heilig et al (59) by a second isolation of the t(X;21 ) junction followed by
cos mid walking (Heilig walk-Figure 3). The probe P20 was isolated by
Wapenaar et al ( 1 23) from a cosmid library of a hamster-human hybrid cell
carrying a part of the X-chromosome short a and mapped into the DMD
gene. The clone GMGXl l was isolated by Gillard (46) from a fow-sorted X
library and mapped into the DMD gene.
The initial DXS20610cus of 120 kb (left side of Figure 3) was extended to
include exons 3-7 (middle of Figure 3) by using cDNA probes to identify
exon-containing cos mid clones covering 230 kb. To date the map between
exons 1 and 3 remains incomplete.
MUTATION ANALYSIS AND CLINICAL APPLICATIONS
Localization and cloning of the gene immediately allows for the study of the
nature of mutations in the gene, and the application of this knowledge to
carrier identification and prenatal diagnosis.
Nature of Mutations in the DMD Gene
Without doubt, the major form of mutation in the gene is deletion. Not only
have large deletions encompassing two or more genes been instumental in
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 61 3
mapping several genes to band Xp21, but intragenic deletion i s the most
common cause of DMD/BMD (33, 41 , 82) . The deletions do not occur
uniformly over the gene: In the DXS164IDXS206 region the frequency is
below 10% (57, 85, 1 1 8), whereas deletions near the middle of the gene
detected with cDNA probes (41 , 82) or with probe P20 ( 124) occur with a
higher frequency. A total of 104 patients in Kunkel's laboratory (82) and an
additional 130 patients in our own laboratory were studicd with eDNA probes
covering the entire gene. Our own data are presented in Figure 4 and clearly
reveal the nonrandomness of the deletions on the eDNA map. The clustered
deletions that begin in one of three introns near 6. 7 kb on the eDNA map have
not been characterized in detail . A realistic interpretation is that the introns
contain sequences that predispose to rearrangement (82). The alterative
explanation that the introns are extraordinarily large appears untenable since
the deletion breakpoints are clustered into a 25-40 kb interval of the genomic
map ( 1 24).
Deletions appear to occur with approximately equal frequency in DMD and
the milder BMD (41 , 57). Sequences deleted in DMD patients may also be
deleted in BMD patients, and deletion size does not correlate with the severity
of the disease (32, 57, 90, 93). An attractive hypothesis is that DMD results
largely from frameshift deletions while BMO usually results from deletions
that maintain the translational reading frame. It has been possible to test the
hypothesis since the intron-exon boundaries are know for the first 20 exons
(95, 97), so that deletions confined to this region may be classified as
frameshift or nonframeshift. Analysis of 3 OMO and 3 BMO patients by
Monaco et al supported the hypothesis (97). In contrast, our own data on 29
patients do not support such a simple model (95), since several mild BMO
patients had frame shif deletions of exons 3-7. The possibility that functional
protein might be produced by re-initiation from an initiation codon in exon 8
was suggested (95).
Another type of mutation, much less common than deletion, is intragenic
duplication (72). Those analyzed to date in our laboratory (Figure 4) appear
to duplicate one or a few exons by tandem duplication of a portion of the
gene, presumably by unequal crossing over between repetitive elements
(72).
Deletions and duplications have not been recognized in affected females,
except in one female with a 45,X chromosome constitution who had a
deletion within the locus (20). Presumably such mutations in heterozygotes
would not be expressed. The mutations that are expressed in females are the
translocations discussed earlier, and many of these have now been shown to
break within the DMD gene (Figure 3) (reviewed in 10).
To date no point mutations or splice junction mutations have been identi
fied, but this might simply relate to the overwhelming task of finding such
mutations in a 2000-kb gene.
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
614 WORTON & THOMPSON
XJ LH1
.
130 patients
68 deletions
8 duplications
.
cDNA 13
97
3 bp
5' 11II11111111 ||| || | | | || |I | | |1 1111 11 1A1 111 1 1 ||1 | |||||111 ||| | | | | 1
3
protein 3
6
8
5
@
N2_i1i2h1
5
i
6
1
7
1a1
9
11q III @ 1II10PIII b @ IcoH
tClln-blndlng lr0tehtcot segments cyslelO-nch C-lermlOol
domIn __________ = |?^m ________ domon domoln
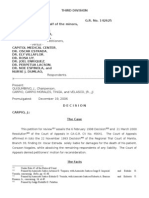
Figure 4 Schematic of the cDNA and the protein product, dystrophin.
A. The 1 3,973 bp cDNA is shown with its 69 or morc cxons. The first 2 1 exons have been
characterized in detail , and the exons are drawn to scale (83, 95) . The remaining exons are
approximations redrawn from Koenig et al (82). Above the exon map the heavy bars delineate the
extent of eight duplications detected among 1 30 DMD patients examined in our laboratory (72).
The thin bars delineate the extent of 68 deletions among the same 130 patients. The spectrum of
deletions, with large deletions typically found in the first third of the gene and a large number of
smaller deletions clustered in the middle of the gene, is remarkably similar to the patter found by
Koenig et al (82) for an independent set of 1 03 patients. Below the exon map is a schematic of the
primary structure of the 3685 amino acid protein taken from Koenig et al (83). The dark block
near the amino terminus is the region of alpha actinin homology with a potential actin-binding
domain. The next domain contains the 26 spectrin-like repeats, some of them numbered. The
margins of the first six repeats coincide with exon boundaries, with one, two, or three exons
encoding one repeat unit (83) . The third domain is the high cysteine region with the potential
Ca2+ binding sites (EF hands) (83). The last domain has no distinguishing features and no
homology to known protcins (83).
I
B. The predicted tertiary structure of the protein (photograph reproduced from Cell, with
permission) (83) . The similarity to cytoskeletal proteins is discussed in the text.
Carrier Identiication and Prenatal Diagnosis
Molecular analysis is now indispensable for carrier/noncarrier identification
and prenatal diagnosis in DMD and BMD. The primary molecular diagnostic
method has been by linkage analysis with genomic probes that recognize
polymorphisms within and fanking the gene. The many such probes that have
been identified, some of which are shown in Figure 1, allow tracing of the
DMD region of the X chromosome through most families and identification of
many deletions and recombinations. Recently cDNA probes, which allow
direct detection of virtually all deletions, have become available.
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 61 5
Intragenic deletions are revealed by failure of probes to hybridize with
genomic DNA. So far, with a single possible exception (84) , males found to
have intragenic deletions have been affected. With current technology it is
possible but difficult to distinguish in females between homozygosity and
hemizygosity for a marker on the basis of the intensity of the hybridization
signal , but presence of a single marker at a site where heterozygosity is
expected unambiguously reveals a deletion.
In several large studies it has been shown that the great majority of women,
even those who have only one affected relative and normal CK activity, can
now be classified as carriers or noncarriers with greatly improved accuracy
over that attained by pedigree analysis and CK assay alone. Use of intragenic
probes as well as fanking probes adds considerably to the likelihood of
finding informative markers and thus of changing an ambiguous estimate of
carrier risk to the upper or lower limit of the risk range (l a, 22, 42, 49, 60,
62, 92, 94) .
When a family has only a single affected male (by far the most common
situation), it may be impossible to determine whether the mother is a carrier or
the patient a new mutant, but prenatal exclusion may still be possible on the
basis of which maternal chromosome has been transmitted to the fetus.
Similarly, a sister of a deceased male may be ofered prenatal exclusion if her
parents' markers are known, since the risk to her fetus travels with her
maternal markers.
When a woman is a carrier and has informative flanking markers of known
linkage phase, prenatal diagnosis is possible with up to 99% accuracy as long
as there has been no recombination in the region flanked by the probes during
maternal meiosis. Recombination, which occurs in a significant proportion of
cases, prevents accurate prediction of the fetal genotype because of the
relatively low level of resolution of analysis by linked markers and the known
heterogeneity of mutation sites within the locus. Darras and colleagues (28)
have emphasized the unavoidable uncertainties in the use of linkage, describ
ing a case in which double recombination, which is undetectable, led to the
birth of an affected child who had been judged to have a low risk. Such an
unfortunate conclusion reflects a limitation inherent in the technique.
Difficulties may also be encountered when DNA from family members
important to the anal ysis cannot be obtained. For example, a patient may be
deceased by the time his sister presents for prenatal diagnosis, fathers impor
tant to the analysis may not be available, or paternity of female family
members may not be as reported. Additional problems include the length and
expense of the procedure (29) , especially if the search for informative markers
is not initially successful .
The recent isolation of cDNA clones offers the possibility of direct prenatal
diagnosis in the large proportion of families in which a deletion mutation is
present, without the need for extensive family studies or the risk of undetected
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
61 6 WORTON & THOMPSON
recombination (29). This approach is likely to be widely used for prenatal
diagnosis in families with deletion mutations because it is not only highly
reliable, but potentially faster and more economical than linkage analysis.
Deletion testing with cDNA probes requires Souther blot analysis with a
minimum of six cDNA probes, each detecting 1 0 or more bands on a blot.
The use of a polymerase chain reaction (PCR) to amplify specific exons that
may then be detected by gel electrophoresis without the need for blotting,
without 32p, and without autoradiography holds great promise for a complete
gene analysis in lcss than one day from receipt of the sample (J. S. Chamber
lain, personal communication). The time required for the analysis is important
since prenatal diagnosis for DMD is preferably performed by chorionic villus
sampling, with a view to termination of pregnancy in the first trimester if the
fetus is an affected male.
Germinal mosaicism, rarely described for other human disorders, may not
be uncommon in DMD/BMD. In several reported pedigrees a parent without a
deletion in somatic cell DNA has nevertheless transmitted an X chromosome
with a deletion to more than one offspring (2, 26, 87, 1 30) . The most likely
possibility is that the transmitting parent is a mosaic with different cell lines
present in somatic and germinal tissues, and mosaicism of the germinal tissue
itself has been reported (26, 1 30) . Though germinal mosaicism has important
genetic implications, its incidence and therefore its significance for genetic
counseling is still unknown. At this time, if an affected boy has a deletion that
is not present in his mother's somatic cells, the mother and her first-degree
female relatives cannot be assumed to be noncarriers; and they should still be
ofered carrier testing and prenatal diagnosis (26).
Unfortunately, carrier detection and prenatal diagnosis, even by the most
efective techniques, do little to reduce the overall incidence of DMD, since
most patients are the only affected members of their families. A step that can
help to reduce the incidence is neonatal screening, which offers a means of
prevention of the birth of second afected boys in kindreds. At present, about
1 0% of DMD patients are second cases in their families, bor before the
disease is expressed in an older close relative. Neonatal screening for DMD
and BMD is feasible and is in use in some areas (51, 1 1 2). Population sceening
for heterozygotes, which could also aid in prevention, is not possible at present.
Neonatal screening for DMD is criticized by some on ethical grounds because no
treatment is available. If amelioration of this tragic disease becomes possible,
neonatal screening will be much more widely accepted.
DYSTROPHIN, THE PROTEIN PRODUCT OF THE DMD
GENE
The long-term goal of the molecular genetic approach has been to use the gene
as a stepping stone to the protein and thus to an understanding of the disease.
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 61 7
The recognition that the DMD gene encodes a large protein triggered early
speculation that nebulin, a large MW protein of the muscle sarcomere, might
be the gene product (129) . However, the finding of a normal amount of
nebulin in dystrophic muscle tissue ( 1 17) and the recent mapping of nebulin
cDNA sequences to chromosome 2 ( 1 1 5) eliminated this possibility.
Once the DMD gene had been cloned it became possible to examine the
gene expression and the protein product more directly, seeking clues to
possible function.
Expression of the DMD Gene
Norther blot analysis with the initial cDNA clones confirmed that the gene
was expressed in fetal and adult human skeletal muscle, but not in skin
fibroblasts or cultured myoblasts ( 1 2, 100). Further studies have revealed that
the gene is expressed in myogenic cell cultures only after the formation of
multinucleated myotubes (89, 1 06), suggesting that the gene product is
important after the onset of terminal differentiation.
Using the more sensitive RNAase protection assay, message has been
detected in rat ( 1 05) and mouse ( 1 8) skeletal muscle, cardiac muscle and
brain, as well as in multinucleated myotubes from a mouse myogenic cell line
and from primary cultures of newborn rat muscle ( 105) . Amplification of
mRNA by the polymerase chain reaction has proved to be a very sensitive
assay and has detected dystrophin message in skeletal, heart, and smooth
muscle, lesser amounts (approximately I % of the amount in muscle) in brain,
kidney, lung, and placenta, and trace amounts (less than 0. 1% of the amount
in skeletal muscle) in liver, spleen, and cultured fibroblasts or lymphoblasts
( 1 9a) .
In our own laboratory the 5' end of the gene has been isolated in a cosmid
clone, and a subclone containing the putative promoter has been tested for
promoter activity in muscle cells. Expression was seen in transfected
myotubes in a standard CAT assay for promoter activity (81).
The level of full-length message i s greatly reduced or absent in patient
muscle (82, 64). However, in some patients at least, message can be detected
by in situ hybridization with a probe from the 5' end of the gene ( 106) . This
message, presumably defective in patents, is particularly prevalent around
the nuclei of regenerating muscle fibers ( 106), consistent with its expression
in fused myotubes in culture.
Dystrophin Structure Deduced from cDNA Sequence
The entire human eDNA and portions of the mouse cDNA for the gene have
been sequenced (24, 64, 82, 83). The human sequence predicts a 427 kd
protein 3685 amino acids in length (Figure 4) . Both DNA and protein
sequence are highly conserved between mouse and human. The deduced
amino acid sequence of the protein, dystrophin, predicts a protein of at least
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
61 8 WORTON & THOMPSON
four domains. The N-terminal domain shows strong sequence homology in
amino acids 14 to 240 to the actin-binding domain of chicken alpha-actinin
(54, 83). The second and largest domain, amino acids 278 to 3080, displays a
weak repeat patter very similar to the repeats found in alpha-actinin and
spectrin (32a, 83). The 1 09 amino acid repeat unit of dystrophin can be
aligned with the 106 amino acid consensus repeat of spectrin, suggesting a
triple helical structure for dystrophin similar to that proposed for spectrin
(32a, 83). The 26 repeat units can be seen in the schematic of Figure 4A. Over
the first 20 exons, boundaries of the repeat units correspond to exon-intron
borders, suggesting that exon duplication is the evolutionary strategy for
lengthening the protein by adding repeat units. The repeat domain probably
adopts a rod shape (Figure 4B) as it does in alpha-actinin and spectrin, and the
self-assembly of these two proteins into anti-parallel dimers suggests a similar
dimerization for dystrophin (83).
The third domain, amino acids 3080 to 3360, is cysteine-rich and i s
followed by the C-terminal domain of 325 amino acids. The third domain
bears sequence similarity to the C-terminal domain of Dictostelium alpha
actin in (but not chicken alpha-actinin) , which contains two Ca2+ binding sites
in the form of EF-hands (Figure 4B) . The C-terminal domain bears no
similarity to any known protein.
The features of dystrophin are therefore strongly suggestive of a long
rod-like molecule that perhaps binds cytoskeletal actin and performs a struc
tural role in the cell (83).
Localization of Dystrophin in the Muscle Cell
The sequence of the DMD cDNA predicted a protein of 427 kd. Hofman and
colleagues (68) have detected a protein of approximately 400 kd on Wester
blots of mouse skeletal muscle proteins. The antibodies used for the Wester
blot analysis were directed against a denatured fusion protein made in E. coli
from a gene consisting of the bacterial trp E gene fused to cDNA clones from
the mouse equivalent of the DMD locus. These anti-dystrophin antibodies
detected high molecular weight protein in human and mouse skeletal and
cardiac muscle, lesser amounts in smooth muscle, and small amounts i n
brain. Dystrophin was not detectable in the muscle proteins of two afected
boys.
Subcellular localization of dystrophin to the triads of skeletal muscle by
Wester blot analysis of fractionated mouse muscle was reported by Hoffman
and coworkers (67). Dystrophin copurified with the Ca2+ release channel
protein (ryanodine receptor) and the (Ca2+ + Mg2+) ATPase in the heavy
microsomal fraction containing the triads. The triad junction consists of
transverse tubules (invaginations of the sarcolemma) interdigitated between
two terminal cisterac of the sarcoplasmic reticulum (SR) . The triad junction
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 61 9
i s the site where the depolarization signal from the motor neuron activates the
release of Ca2+ from the SR to initiate muscle contraction. Localization of
dystrophin to the triads suggested that it might play a role in anchoring the
triads to the myofibrillar cytoskeleton and that its loss through mutation might
disrupt Ca2+ homeostasis (67).
Studies by Zubrzycka-Gaa in our own laboratory in collaboration with
Karpati at the Montreal Neurological Institute have led to somewhat diferent
conclusions ( 1 38). Antibodies prepared against synthetic peptides and native
protein-A fusion proteins derived from human DMD cDNA clones also
recognize a 400-kd muscle protein that is absent from affected boys ( 1 38).
Microscopic localization of dystrophin using indirect avidin-biotin based
immunoperoxidase or immunofuorescence on cryostat sections of human
muscle has revealed a staining patter confined to the sarcolemma of myofi
bers. No intracellular staining has been seen in transverse or cross sections,
indicating a reduced amount of immunoreactive protein in the triads. Since
these fusion protein antibodies were directed at the same portion of the protein
as those of Hofman, and since similar results are obtained with peptide
antibodies directed against amino acid sequences derived from Kunkel's
original cDNA clone ( 1 38), the cytological data are in some disagreement
with the biochemical fractionation data. Since T tubules are invaginations of
the surface membrane it is possible that some dystrophin is located along the
T tubular system, although the major concentration appears to be at the outer
membrane. A similar membrane localization of dystrophin has been achieved
with antibody directed against another synthetic peptide derived from Kunk
el' s cDNA sequence ( 1 , 1 16) and electron microscopy with immunogold
labelled antibody has suggested that the major distribution of dystrophin is on
the cytoplasmic face of the muscle plasma membrane ( 1 24a). The cytological
evidence, if correct, suggests that dystrophin plays a structural role at the
sarcolemma, and that Duchenne and Becker muscular dystrophy are the result
of muscle membrane instablility related to dystrophin insufciency. The
localization of dystrophin to a membrane component and its putative function
of stabilizing the membrane (66, 1 3&) are entirely consistent with the model
of a large cytoskeletal protein. Whether the protein passes through the mem
brane or attaches to some other transmembrane protein is a matter for specula
tion and experimentation.
Pathogenesis of the Disease
Clearl y, DMD and BMD represent a spectrum of disease resulting from
dystrophin insufciency. Wester blot analysis of protein from muscle biop
sies of 103 patients with various neuromuscula disorders has revealed that
dystrophin is not detectable in most severe DMD patients, is present in low
amount in some patients with an intermediate phenotype, and is present but
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
620 WORTON & THOMPSON
altered in molecular weight in most BMD patients (65). Normal dystrophin
was found in patients with 20 other neuromuscular disorders . The absence of
dystrophin from muscle of DMD patients and its reduced staining intensity i n
muscle of BMD patients has also been seen by immunocytochemistry ( 1 ,
1 38).
Further work is still needed to correlate the phenotype of BMD, DMD, and
intermediate phenotype ("outlier") patients with their specific mutations . A
deletion of most of the putative actin-binding domain in mildly affected BMD
patients raises a question about the importance of this domain (83). Another
mildly affected BMD patient with a deletion of at least nine exons from the
spectrin-like repeat .domain suggests that some deletions may have minimal
effect on the conformation of the protein (24). As described in an earlier
section, a model of frameshif deletions in DMD resulting in protein chain
termination and non-shifing deletions in BMD resulting in a mutant protein
with intact ends ( 1 28) is not appl icable to all cases (95).
Mutations within the locus may cause forms of muscular dystrophy other
than typical DMD and BMD. A mild nonprogressive myopathy in one of two
brothers with a complex phenotype including glycerol kinase deficiency and
congenital adrenal hypoplasia has been found to result from a deletion extend
ing into the distal (3 ' ) end of the DMD gene (27). Further phenotypic
diferences in the myopathy produced by unusual deletions or other mutations
of different regions of the gene remain to be explored.
Animal Models
A complete analysis of the pathogenesis of the disease, including possible
pharmacological treatments or gene therapy, will require animal models.
Though the md gene of the mouse appears to be homologous to the DMD
gene, the murine disorder is mild and transient rather than severe and pro
gressive (68) . The equivalence of md and mouse DMD (mDMD) has been
based on the mapping of the mDMD gene to the same region of the chromo
some as mdx ( 1 1 , 1 7, 58) . The human equivalent of this region of the mouse
chromosome contains the gene for Emery-Dreifuss muscular dystrophy
(EDMD) (58, 1 35) , although in humans EDMD maps at the opposite end of
the chromosome from DMD (61 ) . A reduced level of DMD mRNA and
mouse dystrophin in md mice provides the strongest argument that mdx is the
mDMD gene ( 1 8, 64). However, conclusive proof of a detectable lesion in the
mDMD gene in mdx mice is still lacking. Furthermore, Grant and colleagues
(50) report a low level of recombination between md and mDMD which they
interpret as proof of non-identity. One might argue that these are intragenic
recombination events analogous to such events in the human DMD gene
( 1 19), were it not that the recombinants map md and mDMD on opposite
sides of the C-8 (factor VIII) and Rsvp (color blindness) loci (50). The
resolution of this apparent contradiction awaits further experimentation.
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 621
If mdx mice are mutant in the mDMD gene, confirming the validity of the
md model, then the reason for the mild and transient phenotype in the mouse
may hold an important clue to understanding the severity of the human
disease. One possibility is that the lack of dystrophin is most traumatic in
large caliber muscle fibers where the mechanical strain per unit surface area is
the greatest (76) . In mice, where few fibers grow to a diameter greater than
20-25 Jm, the effects of the disease are minimized (76) . This is consistent
with the fact that in DMD patients, the muscles with small caliber fibers
(extraocular, laryngeal) are spared from the segmental necrosis, and in
affected boys with growth hormone deficiency the course of the disease is
considerably milder ( 1 36). Fast muscle fibers appear to be preferentially
affected ( 1 25), although the biological implications of this are not yet clear.
Another animal model that may make it possible to test the relationship
between muscle fiber size and severity of disease is the X-linked muscular
dystrophy of the dog. This disorder resembles DMD clinically and appears to
involve a deficiency in the dog dystrophin gene (23). The opportunity to
transfer the gene to larger and smaller breeds of dogs should provide evidence
for or against the fiber size model, and the very existence of the dog model
provides opportunities for therapeutic trials that may prove to be of im
portance for the human disease.
APPLICA TIONS OF REVERSE GENETICS TO OTHER
DISEASES
There are many genetic disorders for which the protein altered by the mutation
is completely unknown and others for which there is speculation but no exact
knowledge of the protein. Contiguous gene syndromes and X-linked disorders
seen in female carriers of X/autosome translocations, which have been invalu
able in the reverse genetic approach to muscular dystrophy, are also of proven
or potential value in the search for the products of the normal alleles of other
human disease genes.
Contiguous Gene Syndromes
Therc are several dysmorphic syndromes, each with a wide spectrum of
clinical expression, in which some but not all patients have a specific
cytogenetic abnormality. These include the W AGR complex (Wilms tumor,
aniridia, genitourinary tract malformations, gonadoblastoma, and mental
retardation), Beckwith-Wiedemann syndrome, DiGeorge syndrome, Langer
Giedion syndrome, Miller-Dieker syndrome and retinoblastoma. A deletion
or other mutational event afecting a small segment of DNA containing a
number of adjacent but functionally independent genes is thought to underlie
these disorders and explain their variable expression and irregular genetic
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
622 WORTON & THOMPSON
patter ( 1 1 3) . Analysis of the genes deleted or defective in these syndromes
will be useful in the ongoing quest to understand normal development ( 1 13).
The complex phenotypes associated with Xp2l deletions not only led to
cloning of the DMD gene but have also provided insight into the genetic
organization of one of the first extended chromosomal segments to be an
alyzed in depth. Within this gene cluster, the gene that is abnormal in chronic
granulomatous disease (CGD) has also been cloned ( 1 1 0) using probes de
rived from regions of Xp2l that were absent from the DNA of patient BB (44,
86, 98). Similar approaches have led to the cloning of the retinoblastoma gene
on chromosome 1 3 (45, 88) and are being applied to other disease genes.
The achievement of a detailed map and complete sequence analysis of the
human genome is a project that has caught the imagination of many geneti
cists and, in spite of some skepticism, will undoubtedly be pursued because of
its implications both for basic science and for clinical medicine (71 ) . On a
smaller scale, the ability to analyze DNA samples to look for genes responsi
ble for common genetic defects has obvious clinical applications. The tech
niques of mapping and cloning developed for the analysis of contiguous gene
syndromes are likely to find wide application in genetic medicine.
X/autosome Translocations
Most of the many published examples of X/autosome translocations associ
ated with full manifestation of an X-linked trait in a female are cases of DMD
or BMD (73). Several other disorders have been mapped to regions of the X
chromosome by means of Xlautosome translocations: Aarskog syndrome,
Aicardi syndrome, anhydrotic ectodermal dysplasia, Hunter syndrome, in
continentia pigmenti , Lowe' s syndrome, Menkes syndrome and the TKCR
(torticollis, keloids, cryptorchidism, renal dysplasia) syndrome (30, 63, 75) .
High-resolution chromosome analysis is therefore indicated for any female
manifesting an X-linked trait, as the identification and analysis of a balanced
Xlautosome translocation can both explain the clinical expression and indicate
the gene' s probable map position.
Xlautosome translocations associated with X-linked diseases, like complex
deletion syndromes, are experiments of nature that can be used not only to
map disease loci on the chromosome but also to provide the target for
chromosome walking and mapping in an attempt to fnd and clone the gene.
CONCLUSION
In the few years since the new genetics began to be applied to DMD many of
the theoretical and practical problems associated with the disease have been
solved, or at least have become open to solution. Furthermore, it appears that
answers to the Duchenne problem may extend beyond the disease itself and
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 623
lead to improved understanding of the normal biology of muscle. The ultimate
prospect of alleviation is not yet within reach, but the pace of discovery makes
us hopeful that it is no longer totally beyond our grasp.
Literature Cited
1 . Arahata, K. , Ishiura, S. , Ishiguro, T. ,
Tsukahara, T. , Suhara, Y. , et a!. , 1 988.
Immunostaining of skeletal and cardiac
muscle surface membrane with antibody
against Duchenne muscular dystrophy
peptide. Nature 333: 861-63
l a. Bakker, E. , Bonten, E. J . , De Lange,
L. F. , Veenema, H. , Majoor-Krakauer,
D. , et aI , 1 986. DNA probe analysis for
carrier detection and prenatal diagnosis
of Duchenne muscular dystrophy: a
standard diagnostic procedure. J. Med.
Genet. 23:573-80
2. Bakker, E. , Van Broeckhoven, C. , Bon
ten, E. J., Van de Vooren, M. J . ,
Veenema, H . . et aI, 1 987. Germline
mosaicism and Duchenne muscular dys
trophy mutations. Nature 329:55-6
3 . Bartley, J. A. , Pati l , S . . Davenport, S .
Goldstein, D. , Pickens, J . 1 986. Du
chenne muscular dystrophy, glycerol
kinase deficiency, and adrenal insuffi
ciency associated with Xp2 1 interstitial
deletion. J. Fed. 1 08: 1 89-92
4. Benham, F. J:, Hodgkinson, S. , Davies,
K. E. , 1 984. A glyceraldehyde-3-phos
phate dehydrogenase pseudogene on the
short arm of the human X chromosomes
defines a multigene family. EMBO J.
3: 2635-40
4a. Bertelson, C. J . , Bartley, J. A . Mona
co, A. P. , Colletti-Feener, c. , Fisch
beck, K. , Kunkel , L. M. , 1 986.
Localisation of Xp21 meiotic exchange
points in Duchenne muscular dystrophy
families. J. Med. Genet. 23:531 -37
4b. Bjerglund-Nielsen, L. , Jacobsen, B.
B. , Nielsen, I-M. , Tabor , A. , 1 983.
X;autosome translocation in a girl with
muscular dystrophy. Clin Genet 23: 242
5. Bjerglund-Nielsen, L. , Nielsen, I-M. ,
1 984. Turer' s syndrome and Duchenne
muscular dystrophy in a girl with an
X;autosome translocation. Ann. Genet.
27: 1 73-1 77
6. Bodrug, S. E. , Ray, P. N. , Gonzalez, I .
L. , Schmickel, R. D. , Sylvester, J. E. ,
Worton, R. G. , 1 987 . Molecular analy
sis of a constitutional X-autosome
translocation in a female with muscular
dystrophy. Science 237: 1620-24
7. Bortolini, E. R. , Da Silva, D. M. , Che
quer, R. S. , Vianna-Morgante A. M. ,
Zatz, M. , 1 986. Brief Clinical Report:
Duchenne muscular dystrophy in a girl
with a 45,X/46,XXI47,XXX chromo
some constitution. Am. J. Med. Genet.
25:239-43
8. Boyd, Y. , Buckle, V. J . , 1986. Cyto
genetic heterogeneity of trans locations
associated with Duchenne muscular
dystrophy. Clin. Genet. 29: 1 08-1 5
9. Boyd, Y, Cockbur, D. , Holt, S. , Mun
ro, E., Van Ommen, G. J., Gillard, B. ,
Affara, N. , Ferguson-Smith, M. , Craig,
I . , 1 988. Mapping of twelve Xp2 1
translocation breakpoints with respect to
the locus for Duchenne muscular dystro
phy. Cytogenet. Cell Genet, submitted.
1 0. Boyd, Y. , Munro, E. , Ray, P., Worton,
R. , Monaco, T . et aI , 1 987. Molecular
heterogeneity of translocations associ
ated with muscular dystrophy. Clin. Ge
net. 3 1 :265-72
I I . Brockdorff, N., Cross, G. S. , Cavanna,
J . S. , Fisher, E. M. c. , Lyon, M. F. , et
aI , 1 987. The mapping of a eDNA from
the human X-linked Duchenne muscular
dystrophy gene to the mouse X chromo
some. Nature 328: 1 66-68
1 2. Burghes, A. H. M. , Logan, c. , Hu, X. ,
Belfal l , B. , Worton, R. G. , Ray, P. N. ,
1 987. A eDNA clone from the Duchen
ne/Becker muscular dystrophy gene. Na
ture 328:434-37
1 3. Burmeister, M. , Lehrach, H. , 1 986.
Long-range restriction map around the
Duchenne muscular dystrophy gene. Na
HIC 324:582-85
1 4. Burmeister, M. , Monaco, A. P. , Gil
lard, E. F. , Van Ommen, G. J. B. ,
Affara, N. A. , e t aI , 1 988. A 1 0 mega
base physical map of human Xp21 , in
cluding the Duchenne muscular dystro
phy gene. Genomics, 2: 1 89-202
1 5. Bum, 1 . , Povey, S. , Boyd. Y. , Munro,
E. A. , West, L. , et aI, 1 986. Duchenne
muscular dystrophy in one of monozy
gotic twin girls. J. Med. Genet. 23:494-
500
1 6. Canki, N. , Dutrillaux, B. , Tivadar, I . ,
1979. Dystrophie musculaire de Du
chenne chez une petite fille Porte use
d' une translocation t(X;3)(p21 ;q I 3) de
novo. Ann. Genet 22: 35-39
1 7. Chamberlain, 1 . S. , Grant, S. G. ,
Reeves, A. A. , Mullins, L. J, Stephen
son, D. A. , et aI , 1 987. Regional
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
624 WORTON & THOMPSON
localization of the murine Duchenne
muscular dystrophy gene on the mouse
X chromosome. Som. Cell. Mol. Genet.
1 3:671 -78
1 8. Chamberlain, J. S. , Pearlman, J. A. ,
Muzny, D. M. , Gibbs, R. A. , Ranier, J.
E. , et aI, 1 988. Expression of the murine
Duchenne muscular dystrophy gene in
muscle and brain. Science 239: 1 41 6-1 7
1 8a. Chamberlain, J. S. , Ranier, J. E. ,
Pearlman, J. A. , Farwell, N. J . , Gibbs,
R. A. , et ai . , 1 988. Analysis of Duchen
ne muscular dystrophy gene mutations in
mice and humans. In: Cellular and
Molecular Biology ofMuscle Develop
ment. VCLA Symposia on Molecular
and Cellular Biology, New Series,
Volume 93. Alan R. Liss Inc. , New
York, N. Y. , 1988
19. Chelly, J. , Marlhens, F. , Dutrillaux, B. ,
Van Ommen, G. J . , Lambert, M. , e t ai,
1 988. Deletion proximal to DXS68
locus (LI probe site) in a boy with
Duchenne muscular dystrophy, glycerol
kinase deficiency, and adrenal hypopla
sia. Hum. Genet. 78: 22-27
1 9a. Chelly, J . , Kaplan, J-c. , Maire, P. ,
Gautron, S. , Kahn, A. , 1988. Transcrip
tion of the human dystrophin gene in
human muscle and non-muscle tissues.
Nature 333:858-860.
20. Chelly, J. , Marlhens, F. , Le Marec, B. ,
e t aI, 1 986. De novo DNA microdeletion
in a girl with Turer syndrome and
Duchenne muscular dystrophy. Hum.
Genet. 74: 1 93-96
2 1 . Clarke, A. , Roberts, S. H. , Thomas, N.
S. T. , Whitfield, A. , Williams, J. , Har
per, P. S. , 1 986. Duchenne muscular
dystrophy with adrenal insufficiency and
glycerol kinase deficiency: high resolu
tion cytogenetic analysis with molecu
lar, biochemical , and clinical studies. 1.
Med. Genet. 23:501 -08
22. Cole, C. G. , Coyne, A. , Hart, K. A. ,
Sheridan, R. , Walker, A. , et ai , 19.
Prenatal testing for Duchenne and Be
cker muscular dystrophy. Lancet I :
262-65
23. Cooper, B. J . , Winand, N. J . , Stedman,
H. , Valentine, B. A. , Hoffman, E. P. ,
et al 1988. The homologue of the
Duchenne locus is defective in X-linked
muscular dystrophy of dogs. Nature
334: 1 54-56
24. Cross, G. S. , Speer, A. , Rosenthal, A. ,
Forrest, S. M. , Smith, T. J . , Edwards,
Y., et al . 1987. Deletions of fetal and
adult muscle eDNA in Duchenne and
Becker muscular dystrophy patients.
EMBO J. 6:3277-83
25. Danieli, G. A. , Barbujani, G. , 1 984.
Duchenne muscular dystrophy-Frequen
cy of sporadic cases. Hum. Genet
67:252-56
26. Darras, B. T. , Francke, U. , 1 987. A
partial deletion of the muscular dystro
phy gene transmitted twice by an un
affected male. Nature 329:556- 58
27. Darras, B. T. , Francke, V. , 1 988.
Myopathy in complex glycerol kinase
deficiency patients is due to 3 ' deletions
of the dystrophin gene. Am. J. Hum.
Genet. , 43: 1 26- 30
28. Darras, B. T. , Harper, 1. F. , Francke,
V. , 1987. Prenatal diagnosis and detec
tion of carriers with DNA probes in
Duchenne' s muscular dystrophy. New.
Engl. J. Med. 3 1 6: 985-92
29. Darras, B. T. , Koenig, M. , Kunkel, L.
M. , Francke, V. , 1 988. Direct method
for prenatal diagnosis and carrier detec
tion in Duchenne/Becker muscular dys
trophy using the entire dystrophin
eDNA. Am. J. Med. Genet. , 29: 71 3-26
30. Davies, K. E. , Mandel , J-L. , Weissen
bach, J . , Fellous, M. , 1987. Report of
the committee on the genetic constitu
tion of the X and Y chromosomes.
Cytogenet. Cell Genet. 46:277-3 1 5
30a. Davies, K. E. , Patterson, M. N. , Ken
wrick, S. J . , Bell, M. V. , Sloan, H. R. ,
et aI . , 1 988. Fine mapping of glycerol
kinase deficiency and congenital adrenal
hypoplasia within Xp2[ on the short arm
of the human X chromosome. Am. J.
Med. Genet. 29:557-564
3 1 . Davies, K. E. , Pearson, P. L. , Harper,
P. S. , Murray, J. M. , O' Brien, T. , et ai ,
1983. Linkage analysis of two cloned
DNA sequences flanking the Duchenne
muscular dystrophy locus on the short
arm of the human X chromosome.
Nucleic Acids Res [ I :2303-1 3
32. Davies, K. E. , Smith, T. 1 . , Bundey,
5. , Read, A. P. , Flint, T. , et ai , 1988.
Mild and severe muscular dystrophy
associated wih deletions in Xp21 of the
human X chromosome. J. Med. Genet.
25:9-1 3
32a. Davison, M. D. , Critchley, D. R. ,
[988. A[pha-Actinins and the DMD pro
tein contain spectrin-like repeats. -Cell
52: 1 59-160
33. Den Dunnen, J. T., Bakker, E. , K[ein
Breleler, E. G. , Pearson, P. L. , Van
Ommen, G. J. B. , 1 987. Direct detec
tion of more than 50% of the Duchenne
muscular dystrophy mutations by field
inversion gels. Nature 329:642
34. Dorkins, H. , Junien, C. , Mande[, J. L. ,
Wrogemann, K. , Moison, J. P. , et ai ,
1985. Segregation analysis of a marker
localised Xp2 1 . 2-Xp21 . 3 in Duchenne
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 625
and Becker muscular dystrophy fami
lies. Hum. Genet. 7 1 : 1 03-07
35. Dunger, D. B. , Pembrey, M. , Pearson,
P. , Whitfield, A. , Davies, K. E. , Lake,
B. , Williams, D. , Dillon, M. 1. D. ,
1986. Deletion on the X chromosome
detected by direct DNA analysis in one
of two unrelated boys with glycerol
kinase deficiency, adrenal hypoplasia,
and Duchenne muscular dystrophy. Lan
cet 1 :585-87
36. Emanuel , B. S. , Zackai , E. H. , Tucker,
S. H. , 1 983. Further evidence for Xp21
location of Duchenne muscular dystro
phy (DMD) locus: X;9 translocation in a
female with DMD. J. Med. Genet.
20:461 -63
37. Emery, A. E. H. , 1 986. Methodology in
Medical Genetics. An introduction to
statistical methods. Edinburgh: Chur-
chill Livingstone, pp. 1 03 .
38. Emer, A. E. H. , 1987. Duchenne Mus
cular Dvstrophv. Oxford Univ. Press
39. Engel, A. G. , 1 986. Duchenne dystro
phy. In Myology, ed. A. G. Engel, B.
Q. Banker, New York: McGraw-Hill,
pp. 1 1 85-1 238
40. Fischbeck, K. H. , Ritter, A. W .. Tirs
chwcll, D. L. , Kunkel , L. M, Bertelson,
C. J . , et ai, 1 986. Recombination with
PERT87 (DXSI 64) in families with X
linked muscular dystrophy. Lancet 2:
104
41 . Forrest, S. M. , Cross, G. S. , Speer, A. ,
Gardner-Medwin, D. , Bum, J . , Davies,
K. E. , 1 987 . Preferential deletion of ex
ons in Duchenne and Becker muscular
dystrophies. Nature 329: 638-42
42. Forrest, S. M. , Cross, G. S. , Thomas,
N. S. T. , Harer, P. S. , Smith, T. J . , et
ai, 1987. Effective strategy for prenatal
prediction of Duchenne and Becker
muscular dystrophy. Lancet 2: 1 294-
96
43. Francke, U. , Harper, J. F. , Darras, B.
T. , Cowan, 1 . M. , McCabe, E. R. B. , et
ai, 1 987. Congenital adrenal hypoplasia,
myopathy, and glycerol kinase de
ficiency: Molecular genetic evidence for
deletions. Am. J. Hum. Genet. 40: 21 2-
27
44. Francke, U. , Ochs, H. D. , DeMartin
ville, B. , Giacalone, J . , Lindgren, V. , et
aI, 1 985. Minor Xp2 1 chromosome de
letion in a male associated with expres
sion of Duchenne muscular dystrophy,
chronic granulomatous disease, retinitis
pigmentosa, and McLeod syndrome.
Amer. J. Hum. Genet. 37: 250-67
45. Friend, S. H. , Berards, R. , Rogelj, S. ,
Weinberg, R. A. , Rapaport, J . M. , et al
1986. A human DNA segment with
properties of the gene that predisposes to
retinoblastoma and osteosarcoma. Na
ture 323:643-46
46. Gillard, E. F. , 1988. Molecular analysis
of Duchenne muscular dystrophy and
other Xp mutations using cloned DNA
sequences. PhD Thesis. Univ. Glasgow
47. Gomez, M. R. , Engel, A. G. , Dewald.
G. , Peterson, H. A. , 1977. Failure of
inactivation of Duchenne dystrophy X
chromosome in one of female identical
twins. Neurology 27:537-41
48. Goodfellow, P. N. , Davies, K. E. , Rop
ers, H. H. , 1 985. Report of the com
mittee on the genetic constitution of the
X and Y chromosomes. Human Gene
Mapping 8. Cytogenet. Cell Genet.
40:296-352
49. Goodship, J. , Malcolm, S. , Robertson,
M. E. , Pembrey, M. E. , 1 988. Service
experience using DNA analysis for ge
netic prediction in Duchenne muscular
dystrophy. J. Med. Genet. 25: 14-19
50. Grant, S. G. , Mullins, L. J . , Stephen
son, D. A. , Chapman, V. M . 1988.
Recombination separating the mdx and
Dmd loci on the mouse X chromosome.
Genomics. In press.
5 1 . Greenberg, C. R. , e\ aI. , 1988. Gene
studies in newbor males with Duchenne
muscular dystrophy detected by neonatal
screening. Lancet 2:425-27
52. Greenberg, C. R. , Hamerton, J. L. ,
Nigli, M. , Wrogemann, K. , 1 987. DNA
studies in a family with Duchenne
muscular dystrophy and a deletion at
Xp2 1 . Am. J. Hum. Genet. 41 : 1 28-37
53. Grimm, T. , 1 986. Becker Dystrophy, In
Myology. ed. A. G. Engel, Betty Q.
Banker, New York: McGraw-Hill
54. Hammonds, R. G. , 1 987. Protein se
quence of DMD gene is related to actin
binding domain of alpha-actinin. Cell
5 1 : 1
55. Harper, P. S. , 1982. Carrier detection in
Duchenne muscular dystrophy: A criti
cal assessment. In Disorders of the
Motor Unit. ed. D. L. Schotland, New
York: Wiley, pp. 821-46
56. Hart, K. , Cole, C. , Walker, A. , Hodg
son, S. , Johnson, L. , et aI, 1986. The
screening of Duchenne muscular dystro
phy patients for submicroscopic de
letions. J. Med. Genet. 23:51 6-20
57. Hart, K. A. , Hodgson, S. , Walker, A. ,
Cole, C. G. , Johnson, L. , et ai, 1987.
DNA deletions in mild and severe Be
cker muscular dystrophy. Hum. Genet.
75:281 -85
58. Heilig, R. , Lemaire, C. , Mandel, J. -L. ,
Dandolo, L. , Amar, L. , Avner, P. ,
1987. Localization of the region
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
626 WORTON & THOMPSON
homologous to the Duchenne muscular
dystrophy locus on the mouse X chro
mosome. Nature 32t: 1 6t-70
59. Heilig, R. , Lemaire, C. , Mandel, J. L. ,
1 987. A 230 kb cosmid walk i n the
Duchenne muscular dystrophy gene: de
tection of a conserved sequence and of a
possible deletion prone region. Nucleic
Acids Res. 1 5: 91 29-42
60. Hejtmancik, J. F. , Harris, S. G. , Tsao,
C. C. , Ward, P. A. , Caskey, C. T. ,
1 986. Carrier diagnosis of Duchenne
muscular dystrophy using restriction
fragment length polymorphisms. Neu
rology 3: 1 553-62
61 . Hodgson, S. , Boswinkel, E. , Cole, c. ,
Walker, A. , Dubowitz, V. , Granata, C. ,
Merlini, L. , Bobrow, M. , 1 986. A link
age study of Emery-Dreifuss muscular
dystrophy. Hum. GeneT. 74:409-1 6
62. Hodgson, S. , Walker, A. , Cole, c. ,
Hart, K. , Johnson, L. , et ai, 1 987. The
application of linkage analysis to genetic
counseling in families with Duchenne or
Becker muscular dystrophy. 1. Med.
Genet. 24: 1 52-59
63. Hodgson, S. V. , Neville, B. , Jones, R.
W. A. , Fear, C. , Bobrow, M. , 1 985.
Two cases of X/autosome translocation
in females with incontinentia pigmenti.
Hum. Genet. 71 :231-34
6. Hoffman, E. P. , Brown, R. H. , Kunkel ,
L. M. , 1987. Dystrophin: The protein
product of the Duchenne muscular
dystrophy locus. Cell 5 1 : 91 9-28
65. Hoffman, E. P. , Fischbeck, K. H. ,
Brown, R. H. , Johnson, M. , Medori,
R. , et al, 1988. Dystrophin quality and
quantity determines the clinical severity
of Duchenne/Becker Muscular Dystro
phies. New Eng. 1. Med., 31 8: 1 363-
68
66. Hoffman, E. P. , Hudecki , M. S. ,
Rosenberg, P. A. , Pollina, C. M. , Kun
kel, L. M. , 1988. Cell and fiber-type
distribution of dystrophin. Cell, In
press.
67. Hoffman, E. P. , Knudson, C. M. ,
Campbell, K. P. , Kunkel, L. M. , 1 987.
Subcellular fractionation of dystrophin
to the triads of skeletal muscle. Nature
330: 754-57
68. Hoffman, E. P. , Monaco, A. P. , Feen
er, C. C. , Kunkel, L. M. , 1987. Con
servation of the Duchenne muscular
dystrophy gene in mice and humans.
Science 238: 347-50
69. Hofker, M. H. , Bergen, A. A. B. ,
Skrastaad, M. I . , Bakker, E. , Francke,
U. , et al 1 986. Isolation of a random
cosmid clone, cXS, which defines a new
polymorphic locus DXSI 48 near the
locus for Duchenne muscular dystrophy.
Hum. Genet. 74: 27S-79
70. Hotker, M. H. , Wapenaar, M. c. ,
Goor, N. , Bakker, E. , Van Ommen, G.
J. B. , Pearson, P. L. , 1 985. Isolation of
probes detecting restriction fragment
length polymorphisms from X chromo
some-specific libraries: potential use for
diagnosis of Duchenne muscular dystro
phy. Hum. Genet. 70: 148-56
70a. Holden, J. J. A. , Smith, A. , MacLeod,
P. M. , Masotti, R. , Duncan, A. M. V. ,
1986. Xp21 /autosome translocations.
Clin. Genet. 29:51 6-22.
7 1 . Hood, L. E. , Hunkapiller, M. W. ,
Smith, L. M. , 1987. Automated DNA
sequencing and analysis of the human
genome. Genomics 1 : 201-1 2
72. Hu, X. , Burghes, A. H. M. , Ray, P. N. ,
Thompson, M. W. , Murphy, E. G. ,
Worton, R. G. , 1 988. Partial gene dupli
cation in Duchenne and Becker muscular
dystrophies. 1. Med. Genet., 25:369-
76
73. Jacobs, P. A. , Hunt, P. A. , Mayer, M. ,
Bart, R. D. , 1 98 1 . Duchenne muscular
dystrophy (DMD) in a female with an
X/autosome translocation: Further evi
dence that the DMD locus is at Xp2 1 .
Am. 1 . Hum. Genet. 33: 5 1 3-1 t
74. Kanamori, M. , Morton, N. E. , Fujiki,
K. , Kondo, K. , 1987. Genetic Epidemi
ology of Duchenne muscular dystrophy
in Japan: Classical segregation analysis.
Genet. Epid. 4:425-32
75. Kapur, S. , Higgins, J. V. , De1p, K. ,
Rogers, B. , 1987. Menkes syndrome in
a girl with X-autosome translocation.
Am. 1. Med. Genet. 26:503-1 0
76. Karati , G. , Carpenter, S. , 1 986. Small
caliber skeletal muscle fibers do not suf
fer deleterious consequences of dystro
phic gene expression. Am. 1. Med.
Genet. 25:653-58
77. Kean, V. M. , MacLeod, H. L. , Thomp
son, M. W. , Ray, P. N. , Verellen
Dumouli n, C. , Worton, R. G. , 1986.
Pateral inheritance of translocation
chromosomes in a t(X;21) patient with X
linked muscular dystrophy. 1. Med.
GeneT. 23:491-93
78. Kenwrick, S. , Patterson, M. , Speer, A. ,
Fischbeck, K. , Davies, K. , 1 987.
Molecular analysis of the Duchenne
muscular dystrophy region using pulsed
field gel electrophoresis. Cell 48: 351 -
57
79. Kenwrick, S. J. , Smith, T. J. , England,
S. , Collins, F. , Davies, K. E. , 1988.
Localisation of the endpoints of de
letions in the 5 ' region of the Duchenne
gene using a sequence isolated by
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 627
chromosome jumping. Nucleic Acids
Res. 16: 1 305-1 7
80. Kingston, H. M. , Sarfarazi, M. , Tho
mas, N. S. T. , Harper, P. S. , 1984.
Localisation of the Becker muscular
dystrophy gene on the short arm of the X
chromosome by linkage to cloned DNA
sequences. Hum. Genet. 67: 6-1 7
8 1 . Klamut, H. J . , 1988. Gene expression.
Personal communication
82. Koenig, M. , Hoffman, E. P. , Bertelson,
C. J. , Monaco, A. P. , Feener, C. , Kun
kel, LM, 1987. Complete cloning of the
Duchenne muscular dystrophy (DMD)
cDNA and preliminary genomic organi
zation of the DMD gene in normal and
afected individuals. Cell 50:509-1 7
83. Koenig, M. , Monaco, A. P. , Kunkel, L.
M. , 1988. The complete sequence of
dystrophin predicts of rod-shaped cyto
skeletal protein. Cell, 53: 219-28
84. Koh, J. , Pericak-Vance, M. A. , Yamao
ka, L. M. , Hung, W-Y, Worton, R. G. ,
et ai, 1987. Inherited deletion at
Duchenne dystrophy locus in normal
male. Lancet 2: 1 1 54-55
85. Kunkel , L. M. , Hejtmanclk, J. F, Cas
key, C. T. , Spear, A. , Monaco, A P. , et
aI. , 1 986. Analysis of deletions in DNA
from patients with Becker and Duchenne
muscular dystrophy. Nature 322:73-77
86. Kunkel, L. M. , Monaco, A. P. , Mid
dlesworth, W. , Ochs, H. D. , Latt, S. A.
1985. Specific cloning of DNA frag
ments absent from the DNA of a male
patient with an X chromosome deletion.
Proc. Natl. Acad. Sci. USA 82:4778-82
86a. Kunkel, L. M. , Tantravahi , U. , Eisen
hard, M. , Latt, S. A. , 1 982. Regional
localization on the human X of DNA
segments cloned from flow-sorted
chromosomes. Nucleic Acids Res. 10:
1 557-78.
87. Lanman, J. T. , Pericak-Vance, M. A. ,
Bartlett, R. J. , Chen, J. c. , Yamaoka,
L. , et ai, 1987. Familial inheritance of a
DXSI 64 deletion mutation from a
heterozygous female. Am. J. Hum. Ge
net. 41 : 1 38-4
88. Lee, W. H. , Bookstein, R. , Hong, F. ,
Young, L. J. , Shew, J. Y. , Lee, E. Y,
1 987. Human retinoblastoma suscep
tibility gene: cloning, identification, and
sequence. Science 235: 1 394- 99
89. Lev, A. A. , Feener, C. C. , Kunkel, L.
M. , Brown, R. B. , 1987. Expression of
the Duchenne' s muscular dystrophy
gene in cultured muscle cells. J. Bioi.
Chem. 262: 1 581 7-20
90. Liechti-Gallati, S. , Braga, S. , Hirsiger,
H. , Moser, H. , 1987. Familial deletion
in Becker type muscular dystrophy
within the pXl region. Hum. Genet. 77:
267-68
91 . Lindenbaum, R. H. , Clarke, G. , Patel,
C. , Moncrieff, M. , Hughes, 1. T. , 1979.
Muscular dystrophy in an X; 1 transloca
tion female suggests that Duchenne
locus is on X chromosome short a. J.
Med. Genet. 16: 389-92
92. LindlOf, M. , Kianiinen, H. , Davies, K.
E. , De la Chapelle, A. , 1986. Carrier
detection and prenatal diagnosis in X
linked muscular dystrophy using restric
tion fragment length polymorphisms. J.
Med. Genet. 23:560- 72
93. Lindlef, M. , Kianiinen, H. , Va Om
men, G. J. B. , De la Chapelle, A. ,
1988. Microdeletions i n patients with X
linked muscular dystrophy: molecular
clinical correlations. Clin. Genet. 33:
1 31-39
94. LindlOf, M. , Sistonen, P. , De la
Chapelle, A. , 1987. Linked polymor
phic DNA markers in the prediction of
X-linked muscular dystrophy. Ann.
Hum. Genet. 5 1 : 31 7-28
95. Malhotra, S. , 1988. Phenotype correla
tion. Personal comminication
96. Monaco, A. 0. , Bertelson, C. J. , Col
letti-Feener, c. , Kunkel , L. M. , 1987.
Localization and cloning of Xp21 dele
tion breakpoints involved in muscular
dystrophy. Hum. Genet. 75: 221-27
97. Monaco, A. P., Bertelson, C. J. , Liech
ti-Gallati, S. , Moser, H. , Kunkel, L.
M. , 1988. An explanation for the
phenotypic differences between patients
bearing partial deletions of the DMD
locus. Genomics, In press
98. Monaco, A. P. , Bertelson, C. J. , Mid
dlesworth, W. , Colletti, C. A. , Al
dridge, J. , Fischbeck, K. H. , Bartlett,
R. , Pericak-Vance, M. A. , Roses, A.
D. , Kunkel, L. M. , 1985. Detection of
deletions spanning the Duchenne muscu
lar dystrophy locus using a tightly linked
DNA segment. Nature 31 6: 842-5
99. Monaco, A. P. , Kunkel, L. M. , 1987. A
giant locus for the Duchenne and Becker
muscular dystrophy gene. Trends Genet
3: 33-37
100. Monaco, A. P. , Neve, R. L. , Colletti
Feener, C. , Bertelson, C. J . Durit, D.
M. , Kunkel , L. M. , 1986. Isolation of
candidate cDNAs for portions of the
Duchenne muscular dystrophy gene. Na
ture 323:646- 50
1 01 . Morton, N. E. , Chung, C. S. , 1959.
Formal genetics of muscular dystrophy.
Am. J. Hum. Genet. 1 1 : 360-79
102. Moser, H. , 1984. Duchenne muscular
dystrophy: Pathogenetic aspects and ge
netic prevention. Hum. Genet. 66: 1 7-40
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
628 WORTON & THOMPSON
103. Mostacciuolo, M. L. , Lombardi, A. ,
Cambissa, V. , Danieli, G. A. , Angelini,
C. , 1987. Population data on benign and
severe fors of X-linked muscular
dystrophy. Hum. Genet. 75: 217-20
1 04. Murray, I. M. , Davies, K. E, Harper, P.
S. , Meredith, L. , Mueller, C. R. , Wil
liamson, R. , 1 982. Linkage relationship
of a cloned DNA sequence on the short
arm of the X chromosome to Duchenne
muscular dystrophy. Nature 300:69--71
1 00a. Narazaki, 0. , Hanai, T. , Dcki, Y. ,
Mitsudome, A. , 1985. Duchenne
muscular dystrophy in a female with an
X-autosome translocation. Clin Neural
25:432-36
104b. Nevin, N. C. , Hughes, A. E. , Calwell,
M. Lim, I. H. K. , 1986. Duehenne
muscular dystrophy in a female with a
translocation involving Xp2 1 . J. Med.
Genet. 23: 1 71-73
105. Nudel, D. , Robzyk, K. , Yaffe, D. ,
1 988. The putative Duchenne muscular
dystrophy gene is expressed in differen
tiated myogenic cell cultures and in the
brain. Nature 331 :635
106. Oronzi-Scot!, M. , Sylvester, I. E. , Hei
man-Patterson, T. , Shi, Y. -I. , Fieles,
W. , Stedman, H. , Burghes, A. , Ray,
P. , Worton, R. , Fisehbeek, K. H. ,
1988. Duchenne muscular dystrophy
gene expression in normal and diseased
human muscle. Science 239: 1 41 8-20
107. Pena, S. D. I. , Karpati, G. , Carpenter,
S. , Fraser, F. c. , 1987. The clinical
consequences of X-chromosome in
activation: Duehenne muscular dystro
phy in one of monozygotic twins. J.
Neura. Sci. 79:337-4
1 07a. Perez-Vidal, M. T. , Grau, E. S. ,
Vinas, I. P. , Bayona, T. V. , Rustein,
P. , 1983. Dystrofia muscular tipo
Duchenne en una hembra con una
translocacion equilibrada X/6. Rev.
Neural. (Barcelona) 1 1 : 1 55-58
108. Ray, P. N. , Belfall, B. , Duff, C. ,
Logan, C. , Kean, V. , et ai, 1 985. Clon
ing of the breakpoint of an X;21
translocation associated with Duchenne
muscular dystrophy. Nature 31 8:672-75
108a. Ribeir, M. C. M. , Melaragno, M. I . ,
Schmidt, B. , Brunoni, D. , Gabbai , A.
A. , Hackel, C. , 1 986. Duchenne muscu
lar dystrophy in a girl with an (X; 1 5)
translocation. Am. J. Med. Genet. 25:
231-236
1 09. Rowland, L. P. , 1980. Biochemistry of
muscle membranes in Duchenne muscu
lar dystrophy. Muscle & Nerve 3: 3-20
! l0. Royer-Pokora, B. , Kunkel, L. M. ,
Monaco, A. P. , Goff, S. c. , Newbur
ger, P. E. , et ai, 1986. Cloning the gene
for an inherited human disorder-chronic
granulomatous disease-on the basis of its
chromosomal location. Nature 322:32-
38
I l l . Russo, A. , Barbujani, G. , Mostac
ciuolo, M. L. , Herrmann, F. H. , Spieg
ler, W. I. , et ai, 1987. Sporadic cases in
Duchenne muscular dystrophy-A reap
praisal through segregation analysis of
988 sibships. Hum. Genet. 76:230--235
I l i a. Saito, F. , Goto, I. , Kakiniema, H. ,
Nakamura, F. , Murayama, S. , et aI. ,
1985. High resolution banding study of
an x/4 translocation in a female with
Duchenne muscular dystrophy. Hum.
Genet. 7 1 : 370--371
1 12. Schcucrbrandt, G. , Lundin, A. , Lov
gren, T. , Mortier, W. , 1986. Screening
for Duchenne muscular dystrophy: an
improved screening test for creatine
kinase and its application in an infant
screening program. Muscle & Nerve
9: 1 1-23
1 1 3. Schmickel, R. D. , 1986. Contiguous
gene syndromes: A component of
recognizable syndromes. J. Pediatrics
109: 231-41
1 1 4. Smith, T. I., Wilson, L. , Kenwrick, S.
I. , Forrest, S. M. , Speer, A. , et aI. ,
1987. Isolation of a conserved sequence
deleted in Duchenne muscular dystrophy
patients. Nucleic Acids Res. 1 5: 21 67-74
1 1 5. Stedman, H. , Browning, K. , Oliver, N. ,
Oronzi-Scott, M. , Fischbeck, K. , et ai,
1988. Nebulin cDNAs detect a 25 kilo
base transcript in skeletal muscle and
localize to human chromosome two.
Genomics, 2: 1-7
1 1 6. Sugita, H. , Arahata, K. , Ishiguro, T. ,
Suhara, Y. , Tsukahara, T. , et ai, 1988.
Negative Immunostaining of Duchenne
muscular dystrophy (DMD) and mdx
muscle surface membrane with antibody
against synthetic peptide fragment pre
dicted from DMD eDNA. Prac. Japan
Acad. 64:37-39
1 1 7. Sugita, H. , Nonaka, I . , Itoh, Y. , Asa
kura, A. , Hu, D. H. , et ai, 1987. Is
nebulin the product of the Duchenne
muscular dystrophy gene? Proc. Japan
Acad. 63: 1 07-10
1 1 8. Thomas, N. S. T., Ray, P. N. , Worton,
R. G. , Harper, P. S. , 1 986. Molecular
deletion analysis in Duchenne muscular
dystrophy. J. Med. Genet. 23:509--15
1 19. Thompson, M. W. , Ray, P. N. , Belfall ,
B. , Duff, C. , Logan, c. , 1986. Linkage
analysis of polymorphisms within the
DNA fragment Xl cloned from the
breakpoint of an X; 21 translocation
associated with X linked muscular
dystrophy. J. Med. Genet. 23:54855
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
DUCHENNE MUSCULAR DYSTROPHY GENETICS 629
1 20. Van Ommen, G. J. B. , Berelson, C. ,
Ginjaar, H. B. , Den Dunnen, J. T. ,
Bakker, E. , et ai , 1 987. Long-range
genomic map of the Duchenne muscular
dystrophy (DMD) gene: Isolation and
use of J66 (DXS268), a distal intragenic
marker. Genomics 1 : 329-36
1 2 1 . Van Ommen, G. J. B. , Verkerk, J. M.
H. , Hofer, M. H. , Monaco, A. P. ,
Kunkel , L. M. , et ai, 1 986. A physical
map of 4 million bp around the Du
chenne muscular dystrophy gene on the
human X-chromosome. Cell 47:499-
504
1 22. Verellen-Dumoulin, C. H. , Freund, M. ,
De Meyer, R. , Laterre, C. H. , Frederic,
J . , et ai, 1 984. Expression of an X
linked muscular dystrophy in a female
due to translocation involving Xp2l and
nonrandom inactivation of the normal
X chromosome . Hum. Genet. 67: 1 1 5-
1 9
1 23 . Wapenaar, M. C. , Kievits, T. , Blonden,
L. A. J . , Bakker, E. , Den Dunnen, J.
T. , et ai , 1 987. Hybrid cell-mediated
cloning of a new intragenic sequences
from the 3 ' -region of the DMD gene.
Cytogenet. Cell Genet. In press
1 24. Wapenaar, M. c. , Kievits, T. , Hart, K.
A. , Blonden, L. A. J . , Den Dunnen, J .
T. , et ai , 1988. A deletion hotspot in the
Duchenne muscular dystrophy gene.
Genomics, 2: 10 1-08
1 24a. Watkins, S. c. , Hoffman, E. P. , Slay
ter, H. S. , Kunkel, L. M. , 1 988. Im
munoelectron microscopic localization
of dystrophin in myofibres. Nature
333: 863-866
1 25. Webster, C. , Silberstein, L. , Hays, A.
P. , Blau, H. M. , 1 988. Fast muscle fi
bers are preferentially affected in Du
chenne muscular dystrophy. Cell
52: 503-1 3
1 26. Wilcox, D. E. , Cooke, A. , Colgan, J. ,
Boyd, E. , Aitken, D. A. , e t ai, 1 986.
Duchenne muscular dystrophy due to
familial Xp21 deletion detectable by
DNA analysis and flow cytometry.
Hum. Genet. 73: 1 75-80
1 27. Williams, W. R. , Thompson, M. W. ,
Morton, N. E. , 1 983. Complex segrega
tion analysis and computer-assisted ge
netic risk assessment for Duchenne
muscular dystrophy. Am. 1. Med. Ge
net. 14: 3 1 5-33
1 28. Witkowski, J. A. , 1 988. The molecular
genetics of Duchenne muscular dystro
phy: the beginning of the end? Trends
Genet 4: 27-30
129. Wood, D. S. , Zeviani , M. , Prelie, A. ,
Bonilla, E. , Salviati , G. , et ai, 1 987. Is
Nebulin the defective gene product i n
Duchenne muscular dystrophy? New
Engl. 1. Med. 3 1 6: 1 07-08
1 30. Wood, S. , McGillivray, B. , 1 988. Ger
minal mosaicism in Duchenne muscular
dystrophy. Hum. Genet. 78:282-84
1 3 1 . Woron, R. G. , 1 987. Molecular analy
sis of Duchenne and Becker muscular
dystrophy. BioEssays 7: 57-62
1 32. Worton, R. G. , Burghes, A. H. M. ,
1 987. Molecular genetics of Duchenne
and Becker muscular dystrophies. In
terat. Rev. Neurobiol. 29: 1-75
1 33. Worton, R. G. , Duff, c. , Sylvester, J.
E. , Schmickel, R. D. , Willard, H. F. ,
1984. Duchenne muscular dystrophy in
volving translocation of the DMD gene
next to ribosomal RNA genes. Science
224: 1 447-49
1 34. Yasuda, N. , Kondo, K. , 1 980. No sex
difference in mutation rates of Duchenne
muscular dystrophy. 1. Med. Genet.
1 7: 1 06-1 1
\ 35. Yates, J . R. W. , Affara, N. A. ,
Jamieson, D. M. , Ferguson-Smith, M.
A. , Hausmanowa-Petrusewicz, 1. , e t ai,
1 986. Emery-Dreifuss muscular dystro
phy: localisation to Xq27.3 qter con
firmed by linkage to the factor VIII
gene. 1. Med. Genet. 23:587-90
1 36. Zatz, M. , 1986. Benign Duchenne
muscular dystrophy i n a patient with
growth hormone deficiency: A five year
follow-up. Am. 1. Med. Genet. 24: 567-
72
1 37. Zatz, M. , Vianna-Morgante, A. M. ,
Campos, P. , Diament, A. J . , 1 98 1 .
Translocation (X;6) in a female with
Duchenne muscular dystrophy: Im
plications for the localisation of the
DMD locus. 1. Med. Genet. 1 8:442-
47
1 38. Zubrzycka-Gaam, E. E. , Bulman, D.
E. , Karpati, G. , Burghes, A. H. M. ,
Belfall, B. , e t aI, 1 988. The Duchenne
muscular dystrophy gene is localized in
the sarcolemma of human skeletal mus
cle fibers. Nature, 333:466-69
A
n
n
u
.
R
e
v
.
G
e
n
e
t
.
1
9
8
8
.
2
2
:
6
0
1
-
6
2
9
.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
a
r
j
o
u
r
n
a
l
s
.
a
n
n
u
a
l
r
e
v
i
e
w
s
.
o
r
g
b
y
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
o
f
S
i
n
g
a
p
o
r
e
o
n
0
4
/
2
4
/
1
0
.
F
o
r
p
e
r
s
o
n
a
l
u
s
e
o
n
l
y
.
You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- WHO PartographDocument59 pagesWHO PartographAnonymous 0C4OZmR100% (3)
- Evidence-Based Ways to Reduce Maternal MortalityDocument44 pagesEvidence-Based Ways to Reduce Maternal MortalityJalajarani Aridass100% (1)
- Rafa CVDocument3 pagesRafa CVLou Dy SolisNo ratings yet
- Function of Female Reproductive SystemDocument27 pagesFunction of Female Reproductive SystemShirley Espeña PadolinaNo ratings yet
- Breech PresentationDocument57 pagesBreech PresentationShailendra Yadav100% (2)
- Sanitary PadDocument5 pagesSanitary PadKenneth GohNo ratings yet
- Menard CasesDocument9 pagesMenard CasesMenard BiasuraNo ratings yet
- Py 16096Document9 pagesPy 16096neviNo ratings yet
- CH 3 - Tissue RepairDocument24 pagesCH 3 - Tissue RepairWesam AlTawilNo ratings yet
- Presents: Innovative & Practical Solutions For Dental ImplantsDocument15 pagesPresents: Innovative & Practical Solutions For Dental Implantsnathan1043No ratings yet
- Genetics 9 10Document41 pagesGenetics 9 10Anelya TurgambayevaNo ratings yet
- Guidelines for Private Healthcare EstablishmentsDocument58 pagesGuidelines for Private Healthcare EstablishmentsZaw Moe KhineNo ratings yet
- Poor-Excellent (1-10) Poor-Excellent (1-10) Poor-Excellent (1-10)Document1 pagePoor-Excellent (1-10) Poor-Excellent (1-10) Poor-Excellent (1-10)Dian Sulistya EkaputriNo ratings yet
- Nogales Vs Capitol Medical CenterDocument19 pagesNogales Vs Capitol Medical Centersarguss14No ratings yet
- 008 Uk Geoff Knight Riva Star v2 1Document2 pages008 Uk Geoff Knight Riva Star v2 1api-240710651No ratings yet
- Light and Life 2014 HKDSE High FlyersDocument6 pagesLight and Life 2014 HKDSE High FlyersUcb BioeNo ratings yet
- GP Flyers (Updated)Document2 pagesGP Flyers (Updated)api-252859206No ratings yet
- Kathryn Shepel ResumeDocument2 pagesKathryn Shepel Resumeapi-308652637No ratings yet
- Gaffar Ali Qatar 5.00 YrsDocument4 pagesGaffar Ali Qatar 5.00 YrsHR RecruiterNo ratings yet
- List of Hospitals Gujarat PDFDocument11 pagesList of Hospitals Gujarat PDFVijay ChaudharyNo ratings yet
- Leukemia I To 13Document252 pagesLeukemia I To 13Anel RedzepiNo ratings yet
- Best Dentists in Delhi. ToDocument9 pagesBest Dentists in Delhi. Torohit22221No ratings yet
- Under-Five Mortality in MalaysiaDocument9 pagesUnder-Five Mortality in Malaysiamay88_9833% (3)
- Dr. Alban-ODP 2016 SarcomaDocument37 pagesDr. Alban-ODP 2016 SarcomaAfraDewitaNo ratings yet
- Manual of Referral of Surgical Patients in Family MedicineDocument19 pagesManual of Referral of Surgical Patients in Family MedicinedrmaqsoodaliNo ratings yet
- MakalahDocument15 pagesMakalahWhynera Hendra RestaNo ratings yet
- Experience Limits For First Year Speciaty Training 2019 (The Savvy IMG)Document1 pageExperience Limits For First Year Speciaty Training 2019 (The Savvy IMG)SaurabhNo ratings yet
- Ra 9484 Original Document SignedDocument17 pagesRa 9484 Original Document SignedStudy PlaceNo ratings yet
- Skilled Occupation List (SOL)Document5 pagesSkilled Occupation List (SOL)dewminiNo ratings yet
- Notification BHEL Haridwar Medical Officer PostsDocument5 pagesNotification BHEL Haridwar Medical Officer PostsJeshiNo ratings yet