You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- IELTS Task 1 Writing Band DescriptorsDocument2 pagesIELTS Task 1 Writing Band Descriptorspelosa12345No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Powerpoint Presentation DETECTIVE STORIESDocument38 pagesPowerpoint Presentation DETECTIVE STORIESnatasha_dicecca414350% (2)
- Complete First2 Wordlist ItalianDocument1 pageComplete First2 Wordlist Italiannatasha_dicecca4143No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Hockey Sweater by Roch Carrier TextDocument2 pagesThe Hockey Sweater by Roch Carrier Textnatasha_dicecca4143100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Christmas Carol - CH 4Document2 pagesA Christmas Carol - CH 4natasha_dicecca4143No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- A Christmas Carol - CH 4Document2 pagesA Christmas Carol - CH 4natasha_dicecca4143No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
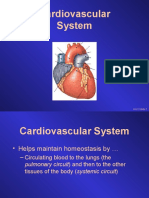
- Cardiovascular System: Unit 3 Slide 1Document79 pagesCardiovascular System: Unit 3 Slide 1Nestor BalboaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Ekg Primeri PDFDocument21 pagesEkg Primeri PDFStevanovic StojaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Acute and Chronic Heart FailureDocument61 pagesAcute and Chronic Heart FailureigohNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Ecg Marrow (Notespaedia) Only@neetpgdiscussion PDFDocument99 pagesEcg Marrow (Notespaedia) Only@neetpgdiscussion PDFanon_1039014600% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 058+ +1595+ +Luh+Made+Indrasuari+ +galleyDocument5 pages058+ +1595+ +Luh+Made+Indrasuari+ +galleyLathief CaakNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Tutorial On Electrophysiology of The Heart) Sam Dudley, Brown UniversityDocument50 pagesTutorial On Electrophysiology of The Heart) Sam Dudley, Brown UniversityNavojit ChowdhuryNo ratings yet
- Tachyarrhythmia SDocument46 pagesTachyarrhythmia SAsif HameedNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Sinus Rhythm DisturbancesDocument3 pagesSinus Rhythm DisturbancesMarcus Philip GonzalesNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Cardiopulmonary ResuscitationDocument163 pagesCardiopulmonary ResuscitationLa Ode RinaldiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- ECG WorksheetDocument3 pagesECG WorksheetElaiza UyNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Introduction of EcgDocument52 pagesIntroduction of Ecgmiss_studyNo ratings yet
- Implantable Cardiac Devices TechnologyDocument123 pagesImplantable Cardiac Devices TechnologyChristoforus D Teach100% (2)
- EKG Interpretasi Dan Lethal Aritmia: Aan NuraeniDocument34 pagesEKG Interpretasi Dan Lethal Aritmia: Aan NuraeniCitra Marchelina Novilini100% (1)
- Obtaining and Interpreting EcgDocument8 pagesObtaining and Interpreting EcgAndra Elena PricopNo ratings yet
- ARRHYTHMIADocument82 pagesARRHYTHMIAjiluNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- List of Mineral Functions and Deficiency Symptoms Followed by The Vitamin & Nutrient Deficiency SymptomsDocument17 pagesList of Mineral Functions and Deficiency Symptoms Followed by The Vitamin & Nutrient Deficiency SymptomsJin Kun Yong100% (1)
- Off Pump CABGDocument8 pagesOff Pump CABGRajat KapurNo ratings yet
- New York Medicaid APG CrosswalkDocument6,734 pagesNew York Medicaid APG CrosswalksdpetesrhsNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- EKG Intermediate Tips Tricks ToolsDocument55 pagesEKG Intermediate Tips Tricks Toolsmayas bsharatNo ratings yet
- PeriarestDocument5 pagesPeriarestMustafa ŠabićNo ratings yet
- EKG InterpretationDocument63 pagesEKG InterpretationMiriam Cindy MathullaNo ratings yet
- 2019 ESC Guidelines For The Management of Patients With Supraventricular TachycardiaDocument3 pages2019 ESC Guidelines For The Management of Patients With Supraventricular TachycardiaBuya TaftaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Multiparametr Simulator PS420 FlukeDocument42 pagesMultiparametr Simulator PS420 FlukeJoséNo ratings yet
- Temporary PacemakerDocument35 pagesTemporary Pacemakerromeorobin07No ratings yet
- Conduction System of Heart and Temporary PacemakerDocument23 pagesConduction System of Heart and Temporary Pacemakersmruti prakash SahuNo ratings yet
- Introduction To ECG For NursingDocument75 pagesIntroduction To ECG For NursingRashid AlHamdan100% (1)
- Podrid's: Ecg EcgDocument392 pagesPodrid's: Ecg EcgMatalus MasterNo ratings yet
- Drug StudyDocument12 pagesDrug StudyCamilley De Vera100% (1)
- Medical Surgical ComprehensiveDocument15 pagesMedical Surgical ComprehensiveMatt Lao DionelaNo ratings yet
- Wesam R KadhumDocument31 pagesWesam R Kadhumwisam_1by1No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)