You might also like
- Environmental ImpactsDocument10 pagesEnvironmental ImpactsIndra DwinataNo ratings yet
- Stata Manual - SEM PDFDocument591 pagesStata Manual - SEM PDFIndra DwinataNo ratings yet
- Learning Outcome of OHOI 2017Document2 pagesLearning Outcome of OHOI 2017Indra DwinataNo ratings yet
- Stata Manual - SEM PDFDocument591 pagesStata Manual - SEM PDFIndra DwinataNo ratings yet
- Perubahan Iklin PDFDocument13 pagesPerubahan Iklin PDFSofiati ClaluNo ratings yet
- Typhoid Stu PDFDocument29 pagesTyphoid Stu PDFIndra DwinataNo ratings yet
- Materi 1. One Health and OHLN OverviewDocument24 pagesMateri 1. One Health and OHLN OverviewIndra DwinataNo ratings yet
- 1 5EpiCurves IssueDocument6 pages1 5EpiCurves IssueRohan Walking TallNo ratings yet
- Topik NSCEDocument1 pageTopik NSCEIndra DwinataNo ratings yet
- Stata RR AllDocument1 pageStata RR AllIndra DwinataNo ratings yet
- 01 - V1-1 - Overview of Outbreak InvestigationsDocument6 pages01 - V1-1 - Overview of Outbreak InvestigationsIndra DwinataNo ratings yet
- 3382 8020 1 CeDocument12 pages3382 8020 1 CeIndra DwinataNo ratings yet
- Artikel 3Document12 pagesArtikel 3Indra DwinataNo ratings yet
- 12: Data Management: Practical Primer Using Epidata. The Epidata Documentation Project. AvailableDocument3 pages12: Data Management: Practical Primer Using Epidata. The Epidata Documentation Project. Availableprsiva2420034066100% (1)
- Kesehatan MasyarakatDocument9 pagesKesehatan MasyarakatIndra DwinataNo ratings yet
- Global CVD AtlasDocument164 pagesGlobal CVD AtlasIndra DwinataNo ratings yet
- Maternal Mortality InfographicDocument1 pageMaternal Mortality InfographicIndra DwinataNo ratings yet
- Appendix3 EQ5D3LDocument2 pagesAppendix3 EQ5D3LIndra DwinataNo ratings yet
- Jurnal MKMI, Vol 6 No.2, Januari 2011, Hal 7-16: Artikel IIDocument10 pagesJurnal MKMI, Vol 6 No.2, Januari 2011, Hal 7-16: Artikel IIIndra DwinataNo ratings yet
- The Ebola WarsDocument21 pagesThe Ebola WarsIndra DwinataNo ratings yet
- 1 5EpiCurves IssueDocument6 pages1 5EpiCurves IssueRohan Walking TallNo ratings yet
- Preface EpiDocument1 pagePreface EpiIndra DwinataNo ratings yet
- Core FETPDocument8 pagesCore FETPIndra DwinataNo ratings yet
- Ebola Case Definition Contact en PDFDocument3 pagesEbola Case Definition Contact en PDFIndra DwinataNo ratings yet
- Organization 1863 1330727586Document4 pagesOrganization 1863 1330727586Indra DwinataNo ratings yet
- Whoqol Hiv Bref PDFDocument5 pagesWhoqol Hiv Bref PDFIndra DwinataNo ratings yet
- Surveillance Workshop Feb 2013-LavigneDocument8 pagesSurveillance Workshop Feb 2013-LavigneIndra DwinataNo ratings yet
- Lepto in ThailandDocument4 pagesLepto in ThailandIndra DwinataNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Reliability of Pulse Palpation in The Detection of Atrial Fibrillation in An Elderly PopulationDocument6 pagesReliability of Pulse Palpation in The Detection of Atrial Fibrillation in An Elderly PopulationAnonymous SWtvkTYGONo ratings yet
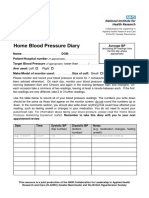
- Home Blood Pressure DiaryDocument2 pagesHome Blood Pressure DiaryCherieNo ratings yet
- Director Emergency Medical Services in Nashville TN Resume Steve FustonDocument2 pagesDirector Emergency Medical Services in Nashville TN Resume Steve FustonSteveFustonNo ratings yet
- Neoplasia ExamDocument9 pagesNeoplasia ExamYheng Gaosaii100% (1)
- Telaah Jurnal KGDDocument17 pagesTelaah Jurnal KGDriska eka fatma HasibuanNo ratings yet
- New Zealand Early Warning Score Vital Sign Chart User Guide 2017Document19 pagesNew Zealand Early Warning Score Vital Sign Chart User Guide 2017Darma YantieNo ratings yet
- DummyDocument13 pagesDummyShellNo ratings yet
- Presentation Transcript: Slide 1Document12 pagesPresentation Transcript: Slide 1khushal2006827088No ratings yet
- Drug AnalysisDocument3 pagesDrug AnalysisAbby BorabienNo ratings yet
- Evidence-Based Nursing: The 5 Steps of EBNDocument13 pagesEvidence-Based Nursing: The 5 Steps of EBNRanjith RgtNo ratings yet
- Soap NoteDocument2 pagesSoap Notetopopirate100% (4)
- Resume 2021Document4 pagesResume 2021api-555218722No ratings yet
- Genu ValgumDocument2 pagesGenu ValgumPurohit_R0% (1)
- Impression TechniquesDocument115 pagesImpression Techniquesandrian_10No ratings yet
- Code of Ethics For NursesDocument6 pagesCode of Ethics For NursesMarianne Jennifer Gan PauloNo ratings yet
- Legalizing MarijuanaDocument3 pagesLegalizing MarijuanaAlyssa MabalotNo ratings yet
- Gastroesophageal Reflux DiseaseDocument9 pagesGastroesophageal Reflux DiseaseNicole Tupayachi ArceNo ratings yet
- Chest PhysiotherapyDocument22 pagesChest PhysiotherapyGhia_Angeles_8457No ratings yet
- Peripheral Nerve InjuryDocument85 pagesPeripheral Nerve InjurySyed Abudaheer100% (3)
- Communication Skills: DR Bob KlajoDocument10 pagesCommunication Skills: DR Bob KlajoBob JohnNo ratings yet
- Statistics Confidence IntervalsDocument3 pagesStatistics Confidence IntervalsCollegestudentNo ratings yet
- Professional Development PlanDocument3 pagesProfessional Development Planapi-385831843No ratings yet
- Manual For Charge NursesDocument99 pagesManual For Charge NursesHazelina Villamor100% (1)
- Pulmonary Tuberculosis Nclex QuestionsDocument3 pagesPulmonary Tuberculosis Nclex Questionssheen100% (6)
- Peptic UlcerDocument5 pagesPeptic UlcerKomal KhanNo ratings yet
- Pelaporan IKP Puskesmas (KAAKP 19 Maret 2022 ArjatyDocument27 pagesPelaporan IKP Puskesmas (KAAKP 19 Maret 2022 ArjatyPutri Kharisma DewiNo ratings yet
- Medical Tourism in IndiaDocument2 pagesMedical Tourism in IndiaDipak Rana0% (1)
- Airway Obstruction Final2Document33 pagesAirway Obstruction Final2Mahindra KumarNo ratings yet
- Reliability and Validity of The Turkish Version of The Job Performance Scale InstrumentDocument9 pagesReliability and Validity of The Turkish Version of The Job Performance Scale InstrumentsatmayaniNo ratings yet
- Hemorrhoids Treatment: All You Need To Know About Hemorrhoids, It's Causes, Symptoms and TreatmentDocument17 pagesHemorrhoids Treatment: All You Need To Know About Hemorrhoids, It's Causes, Symptoms and TreatmentPredrag TerzicNo ratings yet