You might also like
- AAO GoniosDocument43 pagesAAO GoniosmeliabudiNo ratings yet
- Nott Dynamic Retinoscopy: Purpose: To Measure The Accommodative Lag at Near Under Binocular ConditionsDocument2 pagesNott Dynamic Retinoscopy: Purpose: To Measure The Accommodative Lag at Near Under Binocular ConditionsALi SaeedNo ratings yet
- Diseases of LensDocument42 pagesDiseases of LensAmmad ShahidNo ratings yet
- Original Article Factors Related To Filtration-Bleb Morphology After Ex-PRESS SurgeryDocument9 pagesOriginal Article Factors Related To Filtration-Bleb Morphology After Ex-PRESS SurgeryJordi RipollNo ratings yet
- StrabismusDocument45 pagesStrabismusRohit SinghNo ratings yet
- ARCHITECTURAL ANALYSIS OF POST-TRABECULECTOMY BLEB USING AS-OCTDocument18 pagesARCHITECTURAL ANALYSIS OF POST-TRABECULECTOMY BLEB USING AS-OCTSumit Kumar GuptaNo ratings yet
- The Dry EyeDocument8 pagesThe Dry EyeMohit BooraNo ratings yet
- SAP Case Study TemplateDocument105 pagesSAP Case Study TemplateJo KeNo ratings yet
- Binocular Space Perception and Depth CuesDocument20 pagesBinocular Space Perception and Depth CuesKhaled RaquibNo ratings yet
- Chapter 23 Indications and Contradictions For Contact Lens Wear PDFDocument16 pagesChapter 23 Indications and Contradictions For Contact Lens Wear PDFfakenameNo ratings yet
- Brewster StereoscopeDocument17 pagesBrewster StereoscopeNavami KrishnaNo ratings yet
- Trabeculectomy Complications: Characteristics and ManagementDocument31 pagesTrabeculectomy Complications: Characteristics and ManagementalfarizyjefryNo ratings yet
- Types and Treatment of EntropionDocument27 pagesTypes and Treatment of EntropionManu SmrithNo ratings yet
- Advantages and Disadvantages of Aphakics Correction, Types of Aphakic Correction, Problems of Newly Corrected AphakicsDocument78 pagesAdvantages and Disadvantages of Aphakics Correction, Types of Aphakic Correction, Problems of Newly Corrected AphakicsTika100% (1)
- Pricon BroDocument41 pagesPricon Broophtho india inc100% (1)
- The Cornea PPT EditDocument38 pagesThe Cornea PPT EditRahman Setiawan100% (1)
- Fungal KeratitisDocument34 pagesFungal KeratitisbhartiNo ratings yet
- Anatomy of EyeDocument11 pagesAnatomy of EyeAbi Nan ThanNo ratings yet
- Visual SystemDocument37 pagesVisual SystemmalindaNo ratings yet
- GoniosDocument55 pagesGoniosdrquan100% (1)
- PERIPHERAL ULCERATIVE KERATITIS (PUK) AND MOOREN'S ULCER: PATHOGENESIS AND TREATMENTDocument35 pagesPERIPHERAL ULCERATIVE KERATITIS (PUK) AND MOOREN'S ULCER: PATHOGENESIS AND TREATMENTRaissaNo ratings yet
- Panuveitis SAARC - PPT (Autosaved)Document43 pagesPanuveitis SAARC - PPT (Autosaved)Irwan ArziansyahNo ratings yet
- BlepharitisDocument20 pagesBlepharitisNorshahidah IedaNo ratings yet
- Ocular EmergDocument61 pagesOcular EmergKBR RS UNHAS100% (1)
- Retinoscopy and Its Principles: Presenter: DR - Rasika Thakur Moderator: DR - Monica Samant MR - Kunal KishorDocument67 pagesRetinoscopy and Its Principles: Presenter: DR - Rasika Thakur Moderator: DR - Monica Samant MR - Kunal KishorHenok BirukNo ratings yet
- Acute Bacterial Conjunctivitis Treatment and Antibiotic OptionsDocument9 pagesAcute Bacterial Conjunctivitis Treatment and Antibiotic OptionsIka NovitaNo ratings yet
- Binocular Refraction Techniques & AdvantagesDocument17 pagesBinocular Refraction Techniques & Advantageshenok biruk100% (1)
- Laser RetinaDocument70 pagesLaser RetinaSatya Hutama100% (1)
- Visual ImpairmentDocument23 pagesVisual ImpairmentIsrahIzabelPairaAdarnaNo ratings yet
- Capsular Bag Distension Syndrome Following Cataract Surgery JournalDocument16 pagesCapsular Bag Distension Syndrome Following Cataract Surgery Journalnaveen ratna KumarNo ratings yet
- 9893 Alcon Grading Scales 4pp - 0 PDFDocument4 pages9893 Alcon Grading Scales 4pp - 0 PDFDanielle SangalangNo ratings yet
- How to Safely Administer Eye Drops and OintmentsDocument3 pagesHow to Safely Administer Eye Drops and OintmentsDionicia Chandrika0% (1)
- Optometry's Role As A Primary Health Care Provider in Managed CareDocument13 pagesOptometry's Role As A Primary Health Care Provider in Managed CareANDREW OMAKANo ratings yet
- Fluoresce in in OphthalmologyDocument19 pagesFluoresce in in OphthalmologyThingujam JamesNo ratings yet
- 05 Aphakia and PseudophakiaDocument15 pages05 Aphakia and PseudophakiaMwanja Moses100% (1)
- Fundus Fluorescein AngiographyDocument53 pagesFundus Fluorescein AngiographyAnonymous 7uMGcgzXzNo ratings yet
- Introduction To Low VisionDocument15 pagesIntroduction To Low VisionHira AtifNo ratings yet
- Development of Binocular Vision: University of Gondar Department of Optometry by Nebiyat FelekeDocument35 pagesDevelopment of Binocular Vision: University of Gondar Department of Optometry by Nebiyat Felekehenok birukNo ratings yet
- Quality Control in Endoscopy Unit: Safety Considerations For The PatientDocument13 pagesQuality Control in Endoscopy Unit: Safety Considerations For The PatientPamela PampamNo ratings yet
- Eye Test Form 18Document1 pageEye Test Form 18Moisi DragosNo ratings yet
- Retinal Drawing A Lost Art of MedicineDocument3 pagesRetinal Drawing A Lost Art of MedicinekavyaNo ratings yet
- Diseases of Lacrimal ApparatusDocument46 pagesDiseases of Lacrimal Apparatusসপ্নে ছোয়া মন100% (1)
- The GlaucomasDocument29 pagesThe GlaucomasJk FloresNo ratings yet
- NSAIDs: Non-steroidal Anti-inflammatory DrugsDocument45 pagesNSAIDs: Non-steroidal Anti-inflammatory DrugsArvi KhanNo ratings yet
- Episkleritis Dan SkleritisDocument41 pagesEpiskleritis Dan SkleritisSuryana AdityaNo ratings yet
- Where learning is an experience - CVDocument3 pagesWhere learning is an experience - CVabdul87sNo ratings yet
- Corneoscleral T&S - PrinciplesDocument10 pagesCorneoscleral T&S - PrinciplesMuhammad SyamilNo ratings yet
- A Hand Book For Vision Technicians & Primary Eye Care ProvidersDocument79 pagesA Hand Book For Vision Technicians & Primary Eye Care ProvidersFarhan AlleeNo ratings yet
- Large ExotropiaDocument67 pagesLarge ExotropiaTri Kartika UtomoNo ratings yet
- OPTICS Revised + Extra QsDocument75 pagesOPTICS Revised + Extra Qsdoaa naieemNo ratings yet
- Week 11 - Vision Hearing Communication - 20171106Document33 pagesWeek 11 - Vision Hearing Communication - 20171106hkdawnwongNo ratings yet
- Crao PosterDocument1 pageCrao PosterNataShini RajaRatnamNo ratings yet
- Ophtha Case ReportDocument17 pagesOphtha Case ReportJoy Mae Ann PeraltaNo ratings yet
- Brief CGA TemplateDocument3 pagesBrief CGA TemplateMagister Keperawatan GerontikNo ratings yet
- Surgical Management of Senile CataractDocument39 pagesSurgical Management of Senile CataractKarthik ChellaNo ratings yet
- Glaucoma Oral RevalidaDocument11 pagesGlaucoma Oral RevalidaKyle Ü D. CunanersNo ratings yet
- Cogan Syndrome Surger 4, AnkitDocument18 pagesCogan Syndrome Surger 4, AnkitAnkit Tonger AnkyNo ratings yet
- Direct OphthalmoscopeDocument16 pagesDirect OphthalmoscopeMuhammed AbdulmajeedNo ratings yet
- Ocular Manifestations of Thyroid DiseaseDocument20 pagesOcular Manifestations of Thyroid Diseasevivekrajbhilai5850No ratings yet
- TONOMETRY TECHNIQUESDocument49 pagesTONOMETRY TECHNIQUESabhishek tNo ratings yet
- Nord Factory Restore Instructions Edition CDocument1 pageNord Factory Restore Instructions Edition CTonino CannavacciuoloNo ratings yet
- PresiometroDocument25 pagesPresiometrojoseprepaNo ratings yet
- UniversulDocument56 pagesUniversulGabriel DutuNo ratings yet
- Power Theft Identification Using GSM TechnologyDocument3 pagesPower Theft Identification Using GSM TechnologyIJORAT100% (1)
- Iso 10042Document5 pagesIso 10042Nur Diana100% (3)
- ANSYS ACT Developers GuideDocument506 pagesANSYS ACT Developers GuideEDIZONNo ratings yet
- M.E. Comm. SystemsDocument105 pagesM.E. Comm. SystemsShobana SNo ratings yet
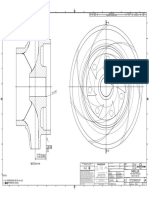
- Impeller: REV Rev by Description PCN / Ecn Date CHK'D A JMM Released For Production N/A 18/11/2019 PDLDocument1 pageImpeller: REV Rev by Description PCN / Ecn Date CHK'D A JMM Released For Production N/A 18/11/2019 PDLSenthilkumar RamalingamNo ratings yet
- Superalloy Brochure PDFDocument16 pagesSuperalloy Brochure PDFDaren NeradNo ratings yet
- UG WeibullDocument776 pagesUG WeibullCharles GuzmanNo ratings yet
- Developmental Morphology and Physiology of GrassesDocument26 pagesDevelopmental Morphology and Physiology of GrassesAnonymous xGVfcqNo ratings yet
- Xenomai 3 DocumentationDocument673 pagesXenomai 3 DocumentationGuile BonafiniNo ratings yet
- c1Document19 pagesc1vgnagaNo ratings yet
- P2 Chp5 RadiansDocument28 pagesP2 Chp5 RadiansWaqas KhanNo ratings yet
- XS Power Batteries D Series InstructionsDocument2 pagesXS Power Batteries D Series InstructionsAutopiezas PanaNo ratings yet
- Metacentric Height: From Wikipedia, The Free EncyclopediaDocument6 pagesMetacentric Height: From Wikipedia, The Free EncyclopediaВладимир ШевченкоNo ratings yet
- Music GcseDocument45 pagesMusic GcseAimee DohertyNo ratings yet
- Design Plan: A Performance Task in GeometryDocument12 pagesDesign Plan: A Performance Task in GeometryRobert Ryan SantiagoNo ratings yet
- Public Key Cryptography: S. Erfani, ECE Dept., University of Windsor 0688-558-01 Network SecurityDocument7 pagesPublic Key Cryptography: S. Erfani, ECE Dept., University of Windsor 0688-558-01 Network SecurityAbrasaxEimi370No ratings yet
- Seminar SPM Additional Mathematics 3472/2: Zuhaila Binti Mohd AliDocument52 pagesSeminar SPM Additional Mathematics 3472/2: Zuhaila Binti Mohd AliIt's nuhaNo ratings yet
- 98 99 Anti Lock BrakesDocument101 pages98 99 Anti Lock BrakestrialnaqueraNo ratings yet
- Solutions To Irodov's Problems - Volume IIDocument442 pagesSolutions To Irodov's Problems - Volume IIZequinha de Abreu100% (2)
- Visualizing Interstellar WormholesDocument14 pagesVisualizing Interstellar WormholesFranciscoNo ratings yet
- VRV A 12 PDFDocument1 pageVRV A 12 PDFMoe Thiri ZunNo ratings yet
- User Mode I. System Support Processes: de Leon - Dolliente - Gayeta - Rondilla It201 - Platform Technology - TPDocument6 pagesUser Mode I. System Support Processes: de Leon - Dolliente - Gayeta - Rondilla It201 - Platform Technology - TPCariza DollienteNo ratings yet
- Wartsila CPP PaperDocument4 pagesWartsila CPP Papergatheringforgardner9550No ratings yet
- Methods For Assessing The Stability of Slopes During Earthquakes-A Retrospective 1Document3 pagesMethods For Assessing The Stability of Slopes During Earthquakes-A Retrospective 1ilijarskNo ratings yet
- CobolDocument224 pagesCobolrahulravi007No ratings yet
- Crystal Chem Crystallography: - Chemistry Behind Minerals and How They Are AssembledDocument33 pagesCrystal Chem Crystallography: - Chemistry Behind Minerals and How They Are AssembledArkodip MandalNo ratings yet
- Ex - No: 4 Integrator and Differentiator Using Fpaa DateDocument4 pagesEx - No: 4 Integrator and Differentiator Using Fpaa DatechandraprabhaNo ratings yet