You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Nursing Care PlanDocument10 pagesNursing Care PlanSittie Rohaina SabanNo ratings yet
- The Client With Urinary Tract InfectionDocument4 pagesThe Client With Urinary Tract InfectionMarisol Jane JomayaNo ratings yet
- CALAS - Module4 All Chapters FINAL2018Document349 pagesCALAS - Module4 All Chapters FINAL2018Muneeb ArshadNo ratings yet
- Experimental Research Chapter 1-3Document16 pagesExperimental Research Chapter 1-3kristleNo ratings yet
- Stool AnalysisDocument11 pagesStool AnalysisMohsen Haleem100% (1)
- Viral Infections of The Gastrointestinal Tract and Viral Infections of The Genitourinary SystemDocument14 pagesViral Infections of The Gastrointestinal Tract and Viral Infections of The Genitourinary SystemDARLENE CLAIRE ANDEZANo ratings yet
- Daftar PustakaDocument2 pagesDaftar Pustakacute_chooeyNo ratings yet
- BacillusDocument18 pagesBacillusdrparachuruNo ratings yet
- Filariasis: Signs and SymptomsDocument30 pagesFilariasis: Signs and SymptomsAnonymous VJjzqbAlNo ratings yet
- Digestive SystemDocument42 pagesDigestive Systemapi-87967494100% (1)
- Kode Diagnosa P-Care - SimpusDocument2 pagesKode Diagnosa P-Care - SimpusiqbalNo ratings yet
- Presepsin Reference Poster 2012Document1 pagePresepsin Reference Poster 2012donkeyendutNo ratings yet
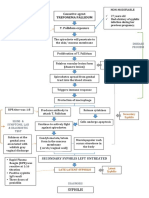
- Path o Physiology of SyphilisDocument1 pagePath o Physiology of Syphilis3S - JOCSON, DENESE NICOLE LEE M.No ratings yet
- Idr 177247 Healthcare Associated Infections An Overview 111418Document13 pagesIdr 177247 Healthcare Associated Infections An Overview 111418ednihs100% (1)
- Systemic Diseases and The EyeDocument17 pagesSystemic Diseases and The Eyeapi-337689057No ratings yet
- Fish Disease BookDocument112 pagesFish Disease BookMemo KenaweeNo ratings yet
- Pathology of The Nervous SystemDocument163 pagesPathology of The Nervous SystemEmmanuel De Leon100% (1)
- Medlifeline Drug of Choice 1st EditionDocument39 pagesMedlifeline Drug of Choice 1st EditionAswin Krishna83% (6)
- DrugsDocument98 pagesDrugsReo PratapNo ratings yet
- Reporting Draft For PPT InputsDocument2 pagesReporting Draft For PPT InputsPhaestus ReverseNo ratings yet
- A& P II Assignment 2Document5 pagesA& P II Assignment 2hepnandeNo ratings yet
- PCV 13Document2 pagesPCV 13api-237098034No ratings yet
- 2015 HBV EQA Result FormDocument3 pages2015 HBV EQA Result FormTiny Coffee HouseNo ratings yet
- Covid 19 RRLDocument2 pagesCovid 19 RRLPurple Ivy GuarraNo ratings yet
- Diaper Rash: What Is Diaper Rash? What Can I Do If My Baby Gets Diaper Rash?Document2 pagesDiaper Rash: What Is Diaper Rash? What Can I Do If My Baby Gets Diaper Rash?gkNo ratings yet
- IBRDocument2 pagesIBRAde HermawanNo ratings yet
- Pest Management Program For Grape Series Downy Mildew of GrapeDocument4 pagesPest Management Program For Grape Series Downy Mildew of Grapeagrosergio2010920No ratings yet
- Self-Assessment Colour Review of Small Animal Soft Tissue SurgeryDocument194 pagesSelf-Assessment Colour Review of Small Animal Soft Tissue Surgerymiliindianu100% (3)
- Nursing Leadership and ManagementDocument7 pagesNursing Leadership and ManagementRamon Carlo AlmiranezNo ratings yet
- Acute Vs Chronic Disease: Comparison ChartDocument3 pagesAcute Vs Chronic Disease: Comparison ChartMoise FloriNo ratings yet