You might also like
- Auerbach's Wilderness Medicine PDFDocument1,672 pagesAuerbach's Wilderness Medicine PDFKieran D90% (10)
- How I Use The Evidence in Dysphagia Management (2) : A Question of TasteDocument3 pagesHow I Use The Evidence in Dysphagia Management (2) : A Question of TasteSpeech & Language Therapy in Practice100% (3)
- Notes in Human Anatomy and PhysiologyDocument9 pagesNotes in Human Anatomy and PhysiologyRikki Mae Bueno100% (3)
- Pre Exam Surgical Notes 2Document166 pagesPre Exam Surgical Notes 2flor vickyNo ratings yet
- Occupational Industrial and Environmental Toxicology, 2nd EditionDocument3 pagesOccupational Industrial and Environmental Toxicology, 2nd EditionTalha AfzalNo ratings yet
- Principles of Molecular Medicine - J. Larry Jamenson - Humana Press - 1998Document1,144 pagesPrinciples of Molecular Medicine - J. Larry Jamenson - Humana Press - 1998BOC100% (1)
- Management of Lower GI BleedDocument48 pagesManagement of Lower GI BleedMegat Mohd Azman AdzmiNo ratings yet
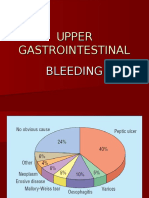
- Upper GIT BleedingDocument69 pagesUpper GIT BleedingSoleh Ramly100% (1)
- An Approach To A Patient With JaundiceDocument48 pagesAn Approach To A Patient With JaundiceSuranga Lakshitha PereraNo ratings yet
- Portal HypertensionDocument4 pagesPortal HypertensiondrstalamNo ratings yet
- Surgical Anatomy-Anal Canal: Dr. Belal MansoorDocument79 pagesSurgical Anatomy-Anal Canal: Dr. Belal MansoorYogi drNo ratings yet
- Biliary Tree LectureDocument58 pagesBiliary Tree Lecturesgod34No ratings yet
- Powerpoint: Disorders of The Thyroid GlandDocument67 pagesPowerpoint: Disorders of The Thyroid Glandj.doe.hex_87100% (1)
- Lower Gi Bleed 4611Document23 pagesLower Gi Bleed 4611Mien BuntaraNo ratings yet
- Upper and Lower Gastrointestinal BleedingDocument36 pagesUpper and Lower Gastrointestinal BleedingDr. Shatdal Chaudhary100% (2)
- Ascites: Pathogenesis and Clinical ApproachDocument34 pagesAscites: Pathogenesis and Clinical ApproachPooja ShashidharanNo ratings yet
- Haemophilia: DR Y S Vishnu Vardhan, PGDocument64 pagesHaemophilia: DR Y S Vishnu Vardhan, PGVishnu Vardhan100% (1)
- 5 MED 4 - Approach To GI BleedingDocument6 pages5 MED 4 - Approach To GI BleedingIan CruzNo ratings yet
- Ascitic Fluid AnalysisDocument3 pagesAscitic Fluid AnalysisLohJNo ratings yet
- Anorectal DiseasesDocument15 pagesAnorectal DiseaseserickNo ratings yet
- Ascites PresentationDocument19 pagesAscites PresentationDanielle FosterNo ratings yet
- Hepato-Biliary System 26.4.2016Document59 pagesHepato-Biliary System 26.4.2016S B SayedNo ratings yet
- Acute Pain Abdomen in Surgical PracticeDocument34 pagesAcute Pain Abdomen in Surgical PracticedrakashnardeNo ratings yet
- PR BleedDocument20 pagesPR BleedCathy KayNo ratings yet
- Pathogenesis of Micro and Macrovascular Complications of DiabetesDocument4 pagesPathogenesis of Micro and Macrovascular Complications of DiabetesFrancesca LiNo ratings yet
- UGIBDocument34 pagesUGIBChe Ainil ZainodinNo ratings yet
- Small Bowel Obstruction: By: Dr. Yasser El Basatiny Prof. of Laparoscopic SurgeryDocument41 pagesSmall Bowel Obstruction: By: Dr. Yasser El Basatiny Prof. of Laparoscopic SurgerydenekeNo ratings yet
- Peptic Ulcer DiseaseDocument20 pagesPeptic Ulcer Diseasedr_IstiqlalMiftahulJannahNo ratings yet
- Interpretation of CBCDocument35 pagesInterpretation of CBCnth1992No ratings yet
- ASCITESDocument25 pagesASCITESGanesh BabuNo ratings yet
- Portal HypertensionDocument65 pagesPortal HypertensionVenu MadhavNo ratings yet
- Ischemic Heart DiseaseDocument28 pagesIschemic Heart DiseaseLiusHarimanNo ratings yet
- Portal Hypertension in Adults - UpToDateDocument12 pagesPortal Hypertension in Adults - UpToDateyessyNo ratings yet
- Approach To Patient With GI BleedDocument22 pagesApproach To Patient With GI BleedZaidatul Atiqah Mustafa100% (1)
- Small Bowel Obstruction - Clinical Diagnosis and TreatmentDocument11 pagesSmall Bowel Obstruction - Clinical Diagnosis and TreatmentVigariooNo ratings yet
- PeritonitisDocument34 pagesPeritonitisabrar_zaidiNo ratings yet
- Endoscopic, Retrograde Cholangio Pancreatography ERCPDocument17 pagesEndoscopic, Retrograde Cholangio Pancreatography ERCPHamzeh AlmasriNo ratings yet
- Upper Gi BleedingDocument35 pagesUpper Gi Bleedingnawriirwan100% (1)
- 9 ThrombosisDocument18 pages9 ThrombosisEslam Almassri100% (1)
- Renal Pathology Blok 13Document71 pagesRenal Pathology Blok 13Arsy Mira PertiwiNo ratings yet
- Gastrointestinal System Block: Case 4BDocument8 pagesGastrointestinal System Block: Case 4BRonald ChrisbiantoNo ratings yet
- Pancreatic Cancer (Cancer of The Pancreas) : Patient Discussions: FindDocument13 pagesPancreatic Cancer (Cancer of The Pancreas) : Patient Discussions: FindMoses ZainaNo ratings yet
- Lower GI BleedingDocument3 pagesLower GI BleedingTaleb AliNo ratings yet
- Lower Gastrointestinal Bleeding (LGIB)Document41 pagesLower Gastrointestinal Bleeding (LGIB)api-196413370% (1)
- Adominal TBDocument50 pagesAdominal TBTamjid KhanNo ratings yet
- Obstructive Jaundice: Dr. SrinivasDocument52 pagesObstructive Jaundice: Dr. SrinivasSahir100% (1)
- LESSON 9 Organ Donation ActDocument56 pagesLESSON 9 Organ Donation ActnullNo ratings yet
- Anorectal Suppuration 9.7.11!1!1Document50 pagesAnorectal Suppuration 9.7.11!1!1Shantu Shirurmath100% (2)
- Hpe CPG Abdominal MassDocument54 pagesHpe CPG Abdominal MassAndri wijaya100% (1)
- Lower GI Bleeding SlideDocument29 pagesLower GI Bleeding Slideraed faisalNo ratings yet
- Abdominal Compartment Syndrome: By: Adel Ghuloom, MD Lubna Kamaldien, MDDocument42 pagesAbdominal Compartment Syndrome: By: Adel Ghuloom, MD Lubna Kamaldien, MDnanang anacardia Subagyo100% (1)
- Renal Failur E: Mamta Kumari Asst - Prof. Igims-ConDocument51 pagesRenal Failur E: Mamta Kumari Asst - Prof. Igims-ConMamta KumariNo ratings yet
- ColonosDocument1 pageColonosVebby 'bee' AstriNo ratings yet
- Surgery II - Pancreas 2014Document20 pagesSurgery II - Pancreas 2014Medisina101No ratings yet
- Surgery 1.1 Fluid and Electrolyte Balance - Azares PDFDocument7 pagesSurgery 1.1 Fluid and Electrolyte Balance - Azares PDFAceking MarquezNo ratings yet
- Jaundice: DR: Ramy A. SamyDocument42 pagesJaundice: DR: Ramy A. Samyoscar3spurgeonNo ratings yet
- HyponatremiaDocument26 pagesHyponatremiaflorenciaii100% (1)
- Chronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDocument42 pagesChronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDon RaulNo ratings yet
- Lower Gastrointestinal BleedingDocument18 pagesLower Gastrointestinal Bleedingosama nawaysehNo ratings yet
- Testicular ExamDocument3 pagesTesticular ExamminikatitingNo ratings yet
- 58 Lower Gastrointestinal BleedDocument4 pages58 Lower Gastrointestinal BleedLuphly TaluvtaNo ratings yet
- Common Histories and Red Flags Presentation Noninteractive VersionDocument21 pagesCommon Histories and Red Flags Presentation Noninteractive VersionesmarNo ratings yet
- Acid-Base Balance 2Document62 pagesAcid-Base Balance 2chimbimbNo ratings yet
- Approach To JaundiceDocument16 pagesApproach To JaundiceMuvenn KannanNo ratings yet
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- Avortul Medicamentos Si ChirurgicalDocument72 pagesAvortul Medicamentos Si ChirurgicalNicu EnachiNo ratings yet
- HIRA ToolDocument26 pagesHIRA Toolsreekala2007No ratings yet
- The Diagnosis and Management ofDocument3 pagesThe Diagnosis and Management ofPreetam PatnalaNo ratings yet
- 5 Weight LossDocument41 pages5 Weight LossTasniiem KhmbataNo ratings yet
- Anatomi Pembuluh Darah KoronerDocument36 pagesAnatomi Pembuluh Darah KoronerenriNo ratings yet
- Surgical Complication of Typhoid FeverDocument10 pagesSurgical Complication of Typhoid FeverHelsa Eldatarina JNo ratings yet
- Medical Emergencies: Oral & Maxillofacial Surgery 1Document7 pagesMedical Emergencies: Oral & Maxillofacial Surgery 1drpnnreddyNo ratings yet
- Neonatology Thesis TopicsDocument7 pagesNeonatology Thesis Topicspwqlnolkd100% (1)
- Pharmacoepidemiology: Origin & EvolutionDocument5 pagesPharmacoepidemiology: Origin & EvolutiongowthamNo ratings yet
- Module 7 Anxiety Disorders PDFDocument12 pagesModule 7 Anxiety Disorders PDFprashansha kumudNo ratings yet
- Katharina Hiria Daundy - Premature Contraction in PregnancyDocument11 pagesKatharina Hiria Daundy - Premature Contraction in PregnancyObgyn AgustusNo ratings yet
- Acute Toxicity: Samson Y RajDocument11 pagesAcute Toxicity: Samson Y RajSamson RajNo ratings yet
- Imaging of Salivary GlandsDocument87 pagesImaging of Salivary GlandsWalaa Mohamed Hamed100% (1)
- Step by Step Root Canal TreatmentDocument157 pagesStep by Step Root Canal TreatmentKaaroma Tamoaieta100% (1)
- World Journal of Radiology PDFDocument8 pagesWorld Journal of Radiology PDFniluhNo ratings yet
- Termorregulacion NeonatosDocument5 pagesTermorregulacion NeonatosMarcela RodriguezNo ratings yet
- Data Sheet ProfalganDocument18 pagesData Sheet Profalganhansen-jcNo ratings yet
- Data Base Bagian Interna Fakultas Muslim Indonesia TAHUN 2021Document17 pagesData Base Bagian Interna Fakultas Muslim Indonesia TAHUN 2021Amalia Azza GhassaniNo ratings yet
- სტაბილური სტენოკარდია - გაიდლაინიDocument59 pagesსტაბილური სტენოკარდია - გაიდლაინიMikheil KakhidzeNo ratings yet
- Perspective: New England Journal MedicineDocument4 pagesPerspective: New England Journal MedicineGary MaoNo ratings yet
- PDS Position Paper On Covid Vaccination - Final - 3 7 21Document7 pagesPDS Position Paper On Covid Vaccination - Final - 3 7 21KROPTECK GNo ratings yet
- Hypertensive Disorders of Pregnancy and AssociatedDocument10 pagesHypertensive Disorders of Pregnancy and AssociatedMedrechEditorialNo ratings yet
- 19 CR 8411 IngDocument1 page19 CR 8411 IngJorge OrtegaNo ratings yet
- Bacterial Skin and Soft Tissue Infections: Clinical Review ArticleDocument9 pagesBacterial Skin and Soft Tissue Infections: Clinical Review ArticleRini MayaSariNo ratings yet
- NIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDocument38 pagesNIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDr mahi sNo ratings yet