You might also like
- Knee Anatomy, Disorders & Osteoarthritis GuideDocument28 pagesKnee Anatomy, Disorders & Osteoarthritis GuideAlisha FatimaNo ratings yet
- Knee DisordersDocument63 pagesKnee Disordersmeto100% (1)
- Sama Notes Upper LimbDocument15 pagesSama Notes Upper LimbMaiUyen Kieu50% (2)
- Case Report OA HipDocument38 pagesCase Report OA HipDian RasitawatiNo ratings yet
- CASE JadiDocument32 pagesCASE JadiDian RasitawatiNo ratings yet
- OVERVIEW: ANATOMY AND PHYSIOLOGY OF ARTHRITIC CONDITIONSDocument43 pagesOVERVIEW: ANATOMY AND PHYSIOLOGY OF ARTHRITIC CONDITIONSGlea PavillarNo ratings yet
- Overview of Anatomy of The Upper LimbsDocument5 pagesOverview of Anatomy of The Upper LimbsRosanaNo ratings yet
- Tugas ReconstructionDocument13 pagesTugas ReconstructionReza Devianto HambaliNo ratings yet
- AnatomyDocument29 pagesAnatomyazeemNo ratings yet
- 3-The Musculosceletal SystemDocument6 pages3-The Musculosceletal SystemEma FröhlichováNo ratings yet
- Lec 14 THE KNEE JOINTDocument17 pagesLec 14 THE KNEE JOINTMaheen IrfanNo ratings yet
- JointsDocument22 pagesJointswazzupwaleedNo ratings yet
- The Anatomy of the Knee Joint: Articulating Surfaces, Ligaments and MovementsDocument7 pagesThe Anatomy of the Knee Joint: Articulating Surfaces, Ligaments and MovementsHassan Mohamed100% (1)
- Musculoskeletal System SummaryDocument7 pagesMusculoskeletal System SummaryFuzna DahliaNo ratings yet
- Anatomy and PhysiologyDocument4 pagesAnatomy and PhysiologyAnnileighjeanNo ratings yet
- BMED 66 - Movement Joints SUMMARYDocument5 pagesBMED 66 - Movement Joints SUMMARYBSMT 1-1, TAN, NICOLE SELINA L.No ratings yet
- 3.arthrology 2010 NewDocument25 pages3.arthrology 2010 Newbenq373No ratings yet
- Knee AnatomyDocument44 pagesKnee AnatomyYanti WijayaNo ratings yet
- JointsDocument27 pagesJointsVarsha Mol MohananNo ratings yet
- O.L.Zharikova, PH.D., Associate Professor Department of Normal Anatomy BSMU, MinskDocument37 pagesO.L.Zharikova, PH.D., Associate Professor Department of Normal Anatomy BSMU, MinsknishaninishaNo ratings yet
- 511-525chapter 6-8 (2) An Introduction To ArticulationsDocument3 pages511-525chapter 6-8 (2) An Introduction To Articulationstomorrow.today.yesterday .yesterdayNo ratings yet
- Orthopaedic SlidesDocument163 pagesOrthopaedic SlidesVivian ChepkemeiNo ratings yet
- Joints: Dr. Vidhya Department of AnatomyDocument27 pagesJoints: Dr. Vidhya Department of Anatomyelan suriyanNo ratings yet
- 1.review OsteoarthritisDocument22 pages1.review OsteoarthritisGERSON RYANTONo ratings yet
- ArticulatioDocument37 pagesArticulatioIshry Ahsani aulia askarNo ratings yet
- Joint Cavity Is PresentDocument9 pagesJoint Cavity Is PresentAlen OsmanovicNo ratings yet
- Case Study LypotDocument16 pagesCase Study LypotlyrenangelicaNo ratings yet
- Persiapan Operasi ORIFDocument38 pagesPersiapan Operasi ORIFamir hamzahNo ratings yet
- Exam 2 Study Guide (1146)Document7 pagesExam 2 Study Guide (1146)S. MartinezNo ratings yet
- Gout Guide: Causes, Symptoms and TreatmentDocument17 pagesGout Guide: Causes, Symptoms and TreatmentPaulette Olisco0% (1)
- Bone tissue functions and remodelingDocument4 pagesBone tissue functions and remodelingIlyasroisulfahmiNo ratings yet
- Theoretical Background of Fibular Tibia Fracture (CrurisDocument21 pagesTheoretical Background of Fibular Tibia Fracture (Crurismutia aNo ratings yet
- Fracture IntroductionDocument21 pagesFracture IntroductionJonathan Delos ReyesNo ratings yet
- Ankylosing SpondylitisDocument17 pagesAnkylosing Spondylitislesliejose1995No ratings yet
- Temporomandibular Joint: DR Bhaumik Thakkar MDS-Part 1. Dept. of Periodontology and ImplantologyDocument60 pagesTemporomandibular Joint: DR Bhaumik Thakkar MDS-Part 1. Dept. of Periodontology and ImplantologyJoseph Eduardo Villar CordovaNo ratings yet
- Interchondral LigamentsDocument8 pagesInterchondral LigamentsAlina MoiseNo ratings yet
- Joint of Lower LimbDocument8 pagesJoint of Lower LimbZaid AbdulqadirNo ratings yet
- Type of JointsDocument51 pagesType of JointsZainab AshroffNo ratings yet
- Bones, Joints, MusclesDocument37 pagesBones, Joints, MusclesQuEycaNo ratings yet
- Muscular and Skeletal SystemDocument8 pagesMuscular and Skeletal SystemPrasad WasteNo ratings yet
- Knee Joint (Anatomy)Document5 pagesKnee Joint (Anatomy)Ojambo FlaviaNo ratings yet
- Medical Surgical Nursing OrthopedicDocument22 pagesMedical Surgical Nursing Orthopedicroger80% (5)
- Examen FisicoDocument26 pagesExamen FisicoAmada Angel VillanuevaNo ratings yet
- Types of Bone Fractures and Clinical ManifestationsDocument10 pagesTypes of Bone Fractures and Clinical ManifestationsFryam BellsNo ratings yet
- Anatomy and PhysiologyDocument4 pagesAnatomy and PhysiologySarah CabalquintoNo ratings yet
- The anatomy and development of the temporomandibular jointDocument13 pagesThe anatomy and development of the temporomandibular jointRajat NangiaNo ratings yet
- TMJ DisordersDocument30 pagesTMJ DisordersDua'a Ma'an100% (3)
- PROJECT KhushbooDocument62 pagesPROJECT KhushbooNitin GuptaNo ratings yet
- The Anatomy and Classification of JointsTITLEDocument43 pagesThe Anatomy and Classification of JointsTITLESadiq Wadood SiddiquiNo ratings yet
- Hard Tissue Replacement-OrthopedicsDocument77 pagesHard Tissue Replacement-OrthopedicsbiomedyuvaNo ratings yet
- Gross Anatomy Learning Objectives - LimbsDocument8 pagesGross Anatomy Learning Objectives - Limbskep1313No ratings yet
- JointsDocument34 pagesJointsNandhana Kattuparambil SunojNo ratings yet
- Knee JointDocument28 pagesKnee JointRaj Shekhar Singh100% (1)
- Pathology of JointsDocument13 pagesPathology of JointswobblegobbleNo ratings yet
- Skeletal and Muscular SystemDocument18 pagesSkeletal and Muscular SystemkimberlynNo ratings yet
- Skeletal SystemDocument104 pagesSkeletal Systemsyafi zulNo ratings yet
- Human Joints and Muscle ClassificationDocument16 pagesHuman Joints and Muscle ClassificationReemNo ratings yet
- WK 2 NFK 202Document88 pagesWK 2 NFK 202JSeasharkNo ratings yet
- Advanced farriery knowledge: A study guide and AWCF theory course companionFrom EverandAdvanced farriery knowledge: A study guide and AWCF theory course companionNo ratings yet
- Improving Ankle and Knee Joint Stability: Proprioceptive Balancefit Discs DrillsFrom EverandImproving Ankle and Knee Joint Stability: Proprioceptive Balancefit Discs DrillsNo ratings yet
- Self Myofascial Release TechniquesDocument6 pagesSelf Myofascial Release Techniquesaslooclt100% (1)
- Win08 MultifidusDocument4 pagesWin08 MultifidusasloocltNo ratings yet
- The John F. Barnes: Myofascial Release ApproachDocument6 pagesThe John F. Barnes: Myofascial Release ApproachasloocltNo ratings yet
- McGuire - UK Sports Symposium Evaluation of Core StabilityDocument8 pagesMcGuire - UK Sports Symposium Evaluation of Core StabilityasloocltNo ratings yet
- MFR Functional TestingDocument0 pagesMFR Functional TestingasloocltNo ratings yet
- Family Violence and Its Impact On Child DevelopmentDocument18 pagesFamily Violence and Its Impact On Child DevelopmentasloocltNo ratings yet
- Soft Tissue Mobilization IntroDocument33 pagesSoft Tissue Mobilization IntroasloocltNo ratings yet
- Back Pain - Chronic IssuesDocument34 pagesBack Pain - Chronic Issuessohrabpk1100% (2)
- Self Myofascial Release TechniquesDocument6 pagesSelf Myofascial Release Techniquesaslooclt100% (1)
- KinesioDocument7 pagesKinesioasloocltNo ratings yet
- TappingDocument53 pagesTappingasloocltNo ratings yet
- 420 Shoulder EvalDocument78 pages420 Shoulder EvalasloocltNo ratings yet
- Human Health and DiseaseDocument40 pagesHuman Health and DiseaseGaurav SharmaNo ratings yet
- Health Education: Věra Kernová National Institute of Public Health PragueDocument23 pagesHealth Education: Věra Kernová National Institute of Public Health PragueasloocltNo ratings yet
- Let's Give Health A Chance: Dr. Rohan BartakeDocument51 pagesLet's Give Health A Chance: Dr. Rohan BartakeasloocltNo ratings yet
- 09balance LabDocument4 pages09balance LabasloocltNo ratings yet
- Fitting Fitness Into A Busy ScheduleDocument14 pagesFitting Fitness Into A Busy ScheduleasloocltNo ratings yet
- Cervical Biomechanics 1Document16 pagesCervical Biomechanics 1leomixkineNo ratings yet
- Effectiveness of Manual Physical Therapy For PainfulDocument10 pagesEffectiveness of Manual Physical Therapy For PainfulasloocltNo ratings yet
- 1 Jeffrey Maitland Spinal Manipulation Made SimpleDocument178 pages1 Jeffrey Maitland Spinal Manipulation Made Simpleaslooclt94% (16)
- 269 270Document50 pages269 270asloocltNo ratings yet
- Management in Physical Therapy PracticeDocument335 pagesManagement in Physical Therapy PracticeasloocltNo ratings yet
- Cervical Biomechanics 1Document16 pagesCervical Biomechanics 1leomixkineNo ratings yet
- ICU Management: - A Physiotherapist'sDocument60 pagesICU Management: - A Physiotherapist'sasloocltNo ratings yet
- Back Pain - Chronic IssuesDocument34 pagesBack Pain - Chronic Issuessohrabpk1100% (2)
- 420 Shoulder EvalDocument78 pages420 Shoulder EvalasloocltNo ratings yet
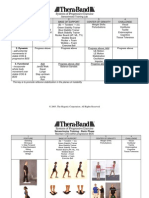
- Systems of Progressive Exercise: BBB: Exercise Ball LabDocument8 pagesSystems of Progressive Exercise: BBB: Exercise Ball LabasloocltNo ratings yet
- Total Knee Replacement ProtocolDocument4 pagesTotal Knee Replacement ProtocolSheel GuptaNo ratings yet
- Tecnica LapradeDocument5 pagesTecnica LapradeThiagoNo ratings yet
- Modul F2 Science Chapter 1Document21 pagesModul F2 Science Chapter 1NorelyanaAli95% (21)
- Build Chest & Triceps Workout RoutineDocument1 pageBuild Chest & Triceps Workout RoutineHarshNo ratings yet
- Lacrimal Duct Anatomy & Obstruction StudiesDocument2 pagesLacrimal Duct Anatomy & Obstruction StudiesWidyastutiNo ratings yet
- SensesDocument45 pagesSenseslouradel100% (1)
- Bates’ Guide to Physical Examination and History Taking Chapter 16: The Musculoskeletal System MCQDocument12 pagesBates’ Guide to Physical Examination and History Taking Chapter 16: The Musculoskeletal System MCQmanesNo ratings yet
- Sced 3204B LDocument5 pagesSced 3204B LEllen Grace Dela PeñaNo ratings yet
- Old School IronDocument9 pagesOld School IronOr83% (12)
- Neurology of Swallowing and DysphagiaDocument24 pagesNeurology of Swallowing and DysphagiaMaríaFernandaCampanoGacitúaNo ratings yet
- نسخة نسخة Final Print Medical TerminologyI Eng 210 LecturesDocument109 pagesنسخة نسخة Final Print Medical TerminologyI Eng 210 LecturesZainab AlhumaidNo ratings yet
- Regenesis 1Document14 pagesRegenesis 1White Light100% (3)
- Principal Veins and ArteriesDocument5 pagesPrincipal Veins and Arteriesrodz_verNo ratings yet
- Head Toe Physical AssessmentDocument2 pagesHead Toe Physical Assessmentzbestgurl100% (2)
- Bulgarian Split Squat Lateral: Lateral LungeDocument47 pagesBulgarian Split Squat Lateral: Lateral LungeZac Brouillette100% (10)
- Power Development Through Complex Training For The.3Document14 pagesPower Development Through Complex Training For The.3PabloAñonNo ratings yet
- Clinical Teaching Birth InjuriesDocument15 pagesClinical Teaching Birth InjuriesAjit M Prasad PrasadNo ratings yet
- Green Operative Hand Surgery - Tendon InjuryDocument2 pagesGreen Operative Hand Surgery - Tendon InjurySamuel Jason0% (1)
- Eustachian Tube Dysfunction Patient InfoDocument2 pagesEustachian Tube Dysfunction Patient InfoAngela Mitchelle NyanganNo ratings yet
- The Nervous SystemDocument39 pagesThe Nervous SystemReizel Mae Noel Laurente100% (1)
- Anatomy and Physiology SystemsDocument21 pagesAnatomy and Physiology SystemsOrmie ChanNo ratings yet
- Shoulder Anatomy GuideDocument37 pagesShoulder Anatomy GuideevelynNo ratings yet
- Seminar on Orthodontic and Orthopedic AppliancesDocument41 pagesSeminar on Orthodontic and Orthopedic AppliancesSibi NairNo ratings yet
- TMD FLDocument189 pagesTMD FLYaser JasNo ratings yet
- Mani 002b8eDocument90 pagesMani 002b8eRuma BhaskerNo ratings yet
- Abdominal Wall: Um-Hani'S Qbank Um-Hani'S QbankDocument5 pagesAbdominal Wall: Um-Hani'S Qbank Um-Hani'S QbankmedisharedNo ratings yet
- Logbook Spring 2023Document98 pagesLogbook Spring 2023Horn Dude100% (1)
- Orthopedic Secrets, 3rd EditionDocument61 pagesOrthopedic Secrets, 3rd EditionPJHG100% (10)
- Try-In of The Trial Denture by Dr. Mahmoud RamadanDocument9 pagesTry-In of The Trial Denture by Dr. Mahmoud RamadanDrRahul Puri GoswamiNo ratings yet
- Volkmann's Ischemic ContractureDocument41 pagesVolkmann's Ischemic ContractureKrishna Madhukar91% (11)
- Neligan Mandible FractureDocument13 pagesNeligan Mandible FractureannisaNo ratings yet