You might also like
- Comparative Study of Oral Swab and Saliva Flora in Patients With Oral Cancer During Chemo - RadiotherapyDocument6 pagesComparative Study of Oral Swab and Saliva Flora in Patients With Oral Cancer During Chemo - RadiotherapyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- AVEED Testosterone Undecanoate UCM348092Document145 pagesAVEED Testosterone Undecanoate UCM348092James LindonNo ratings yet
- Pressure Sensitive Adhesives For Transdermal DeliveryDocument10 pagesPressure Sensitive Adhesives For Transdermal DeliverySadaham SulangaNo ratings yet
- Osmotic Drug Delivery Systems 3Document48 pagesOsmotic Drug Delivery Systems 3anupnakat50% (2)
- DrReddys Annual ReportDocument236 pagesDrReddys Annual Reportpushker_37755No ratings yet
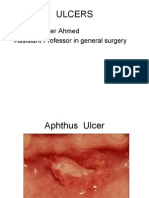
- Apthous Ulcers: Made By: Ammar Raza Roll No. 45Document9 pagesApthous Ulcers: Made By: Ammar Raza Roll No. 45Samiya AnsariNo ratings yet
- Penetration EnhancersDocument17 pagesPenetration EnhancersPharmaosmosis NiperNo ratings yet
- HPEX 358-002 - Basics of EpidemiologyDocument31 pagesHPEX 358-002 - Basics of EpidemiologyMichelle ValenzuelaNo ratings yet
- EMLA Product MonographDocument46 pagesEMLA Product Monographketan79797No ratings yet
- Commonucable Diseases EpidemiologyDocument59 pagesCommonucable Diseases Epidemiologyد.شيماءسعيد100% (1)
- Bacterial Infections of The Oral CavityDocument212 pagesBacterial Infections of The Oral CavitydrrakbdsNo ratings yet
- Infectious Diseases. Etiology PDFDocument76 pagesInfectious Diseases. Etiology PDFIoana CozmaNo ratings yet
- Transdermal Drug Delivery: BackingDocument32 pagesTransdermal Drug Delivery: BackingmurtazaNo ratings yet
- Ulcer, Cyst, Tumoures, Sinus, FistullaDocument40 pagesUlcer, Cyst, Tumoures, Sinus, Fistulladrhiwaomer100% (2)
- New Drug Delivery Systems: A Global OpportunityDocument24 pagesNew Drug Delivery Systems: A Global OpportunityRugun Clara SamosirNo ratings yet
- Find and Record Outbreak CasesDocument37 pagesFind and Record Outbreak CasesHussein Omar Ali 212-41-1419No ratings yet
- l3 Measures of Population Impact and Infectiouness NotesDocument9 pagesl3 Measures of Population Impact and Infectiouness Notestheus_35No ratings yet
- Environmental EpidemiologyDocument5 pagesEnvironmental EpidemiologyKarthik VkNo ratings yet
- Basic Epidemiology Lessons 1 5Document99 pagesBasic Epidemiology Lessons 1 5Khelly Joshua UyNo ratings yet
- Hospital EpidemiologymiologyDocument98 pagesHospital EpidemiologymiologyRizky PebryanNo ratings yet
- Skin Rashes in ChildrenDocument11 pagesSkin Rashes in ChildrenwiladamanikNo ratings yet
- Oral Mucous MembraneDocument36 pagesOral Mucous MembraneFourthMolar.comNo ratings yet
- Osmotic Drug Delivery SystemDocument10 pagesOsmotic Drug Delivery SystemkishoreNo ratings yet
- Medications For Pain and InflammationDocument38 pagesMedications For Pain and InflammationDJJNo ratings yet
- Lecture Notes On Epidemiological Studies For UndergraduatesDocument41 pagesLecture Notes On Epidemiological Studies For UndergraduatespopasorinemilianNo ratings yet
- Dermato ToxicologyDocument1,121 pagesDermato ToxicologyBella LunaNo ratings yet
- Thyroid Scintigraphy-Coass RadiologiDocument29 pagesThyroid Scintigraphy-Coass RadiologiBerlianaiiNo ratings yet
- Brain ScintigraphyDocument24 pagesBrain ScintigraphyDustin Miranda100% (1)
- Orange Book 33rd EditionDocument1,346 pagesOrange Book 33rd EditionIamkoala SiNo ratings yet
- Sunscreen Guide Explains Key ConceptsDocument121 pagesSunscreen Guide Explains Key ConceptsRizweta DestinNo ratings yet
- Floating FilmDocument13 pagesFloating Filmchittam suvarnaNo ratings yet
- 4 Carbohydrates 150929Document53 pages4 Carbohydrates 150929Cahyarani ParamestiNo ratings yet
- Antifungals Topical & Systemic Level IIIDocument16 pagesAntifungals Topical & Systemic Level IIItheintrovNo ratings yet
- Transdermal Drug Delivery SystemDocument47 pagesTransdermal Drug Delivery SystemMridul AroraNo ratings yet
- Insitu Gels PaperDocument7 pagesInsitu Gels PaperShreya100% (1)
- Operations Research: HistoryDocument6 pagesOperations Research: HistoryEdmond DantèsNo ratings yet
- InflammationDocument14 pagesInflammationPrince AhmedNo ratings yet
- Curs Engleza Renal Scintigraphy FinalDocument29 pagesCurs Engleza Renal Scintigraphy FinalIoana MuntianuNo ratings yet
- NCD-Surveillance PPT Final 09132013 PDFDocument49 pagesNCD-Surveillance PPT Final 09132013 PDFNur HusnulNo ratings yet
- Antifungal Drugs: Mechanisms of Action and Clinical UsesDocument70 pagesAntifungal Drugs: Mechanisms of Action and Clinical Usesnk999999No ratings yet
- Transdermal Drug DeliveryDocument18 pagesTransdermal Drug DeliveryIzhal StewartNo ratings yet
- Operational Research by BeeDocument27 pagesOperational Research by BeeabhisakhujaNo ratings yet
- Sampling & Sampling DistributionDocument36 pagesSampling & Sampling Distributionanindya_kundu100% (2)
- Lecture16 PDFDocument27 pagesLecture16 PDFmarkkkkkkkheeessNo ratings yet
- Acute Service Pain Handbook 2011Document116 pagesAcute Service Pain Handbook 2011Iskandar414No ratings yet
- Pai - Lecture4 - Measures of Effect and ImpactDocument54 pagesPai - Lecture4 - Measures of Effect and ImpactAndry KurniadiNo ratings yet
- Fungal Diseases of The Oral MucosaDocument5 pagesFungal Diseases of The Oral MucosaManar AlsoltanNo ratings yet
- Comparision of SCANRDI Vs Pharmacopiea MethodDocument10 pagesComparision of SCANRDI Vs Pharmacopiea MethodUmair ShekhaniNo ratings yet
- Antifungal LectureDocument62 pagesAntifungal LectureVandana TayalNo ratings yet
- Distribution of Sunscreens On SkinDocument7 pagesDistribution of Sunscreens On SkinDouglas DouradoNo ratings yet
- Clinical Trial Course BrochureDocument11 pagesClinical Trial Course BrochurechouguleNo ratings yet
- Calucatiing QALY Comparing QALY and DALY CalculationsDocument7 pagesCalucatiing QALY Comparing QALY and DALY CalculationsmaximussathishNo ratings yet
- Guideline Quality Transdermal Patches enDocument27 pagesGuideline Quality Transdermal Patches endinaNo ratings yet
- Survival Analysis Using SPSSDocument57 pagesSurvival Analysis Using SPSSulisessaldiasroaNo ratings yet
- Factorial Analysis of VarianceDocument20 pagesFactorial Analysis of VarianceRiza Arifianto MarasabessyNo ratings yet
- Physics of Nuclear MedicineDocument90 pagesPhysics of Nuclear MedicineArvindhanNo ratings yet
- National Tuberculosis ProgramDocument37 pagesNational Tuberculosis ProgramDon Oliveros ÜNo ratings yet
- CHN - Communicable DiseaseDocument117 pagesCHN - Communicable DiseaseGetom NgukirNo ratings yet
- Fwd. Epi 8Document40 pagesFwd. Epi 8Sumayya ChughtaiNo ratings yet
- Communicable Diseases ExplainedDocument329 pagesCommunicable Diseases ExplainedCarl WaletNo ratings yet
- Time Table and Time ScheduleDocument1 pageTime Table and Time SchedulePoorny PurushothNo ratings yet
- Computer Short KeysDocument9 pagesComputer Short KeysAliNo ratings yet
- Rajiv Gandhi Unversity of Health Sciences, Bangalore, KarnatakaDocument24 pagesRajiv Gandhi Unversity of Health Sciences, Bangalore, Karnatakamanjugunnal50% (2)
- Rural Health Care System in IndiaDocument30 pagesRural Health Care System in IndiaPoorny PurushothNo ratings yet
- AdoleDocument33 pagesAdolePoorny PurushothNo ratings yet
- Legal and Ethical Issues in NursingDocument2 pagesLegal and Ethical Issues in NursingPoorny PurushothNo ratings yet
- Application For RegistrationfinalDocument2 pagesApplication For RegistrationfinalPoorny PurushothNo ratings yet
- NVBDCPDocument62 pagesNVBDCPPoorny PurushothNo ratings yet
- Mscnregulations 2010 Ver 2Document187 pagesMscnregulations 2010 Ver 2John SamuelNo ratings yet
- India Health PrimerDocument35 pagesIndia Health PrimerPoorny PurushothNo ratings yet
- Rural Health Care System in IndiaDocument30 pagesRural Health Care System in IndiaPoorny PurushothNo ratings yet
- Mscnregulations 2010 Ver 2Document187 pagesMscnregulations 2010 Ver 2John SamuelNo ratings yet
- Tobacco CessationDocument59 pagesTobacco CessationPoorny PurushothNo ratings yet
- SVIMS-No Que-2Document1 pageSVIMS-No Que-2LikhithaReddy100% (1)
- Arp0108 2018Document75 pagesArp0108 2018justin.kochNo ratings yet
- LabyrinthDocument4 pagesLabyrinthAyezaZuberyNo ratings yet
- 8-26-16 Police ReportDocument14 pages8-26-16 Police ReportNoah StubbsNo ratings yet
- IMCI Chart 2014 EditionDocument80 pagesIMCI Chart 2014 EditionHarold DiasanaNo ratings yet
- Venus in MulaDocument2 pagesVenus in MulaGovind BallabhNo ratings yet
- Mufon Ufo JournalDocument21 pagesMufon Ufo JournalSAB78No ratings yet
- EO On Ban of Fireworks (Integrated)Document2 pagesEO On Ban of Fireworks (Integrated)Mario Roldan Jr.No ratings yet
- Allium CepaDocument90 pagesAllium CepaYosr Ahmed100% (3)
- Ethamem-G1: Turn-Key Distillery Plant Enhancement With High Efficiency and Low Opex Ethamem TechonologyDocument25 pagesEthamem-G1: Turn-Key Distillery Plant Enhancement With High Efficiency and Low Opex Ethamem TechonologyNikhilNo ratings yet
- Abstract - Tropen Tag 2011 PDFDocument634 pagesAbstract - Tropen Tag 2011 PDFzmoghesNo ratings yet
- Carpentry Shop: Building, Doors, Windows, Trusses, WorkbenchesDocument105 pagesCarpentry Shop: Building, Doors, Windows, Trusses, WorkbenchesVinod KumarNo ratings yet
- ERS M22 PC4 FerryDocument2 pagesERS M22 PC4 FerryouakgoodNo ratings yet
- Natural Resources in PakistanDocument5 pagesNatural Resources in PakistanSohaib ENo ratings yet
- LH 11 180 190 220 230 270 280 390 400 Breaker Safety & Operating InstructionsDocument304 pagesLH 11 180 190 220 230 270 280 390 400 Breaker Safety & Operating InstructionshadensandorNo ratings yet
- Aging and Elderly IQDocument2 pagesAging and Elderly IQ317537891No ratings yet
- 2-D Motion Based Real Time Wireless Interaction System For Disabled PatientsDocument5 pages2-D Motion Based Real Time Wireless Interaction System For Disabled PatientsSantalum AlbumNo ratings yet
- BCM Continuous ImprovementDocument22 pagesBCM Continuous ImprovementnikoNo ratings yet
- Chapter 4Document26 pagesChapter 4Lana AlakhrasNo ratings yet
- RHS NCRPO COVID FormDocument1 pageRHS NCRPO COVID Formspd pgsNo ratings yet
- Nursing Diagnosis TemplateDocument6 pagesNursing Diagnosis Templatesdk6972No ratings yet
- Social Studies SbaDocument12 pagesSocial Studies SbaSupreme KingNo ratings yet
- Vaginal Examinations in Labour GuidelineDocument2 pagesVaginal Examinations in Labour GuidelinePooneethawathi Santran100% (1)
- Pack Alimentacion Clin in Perin 14Document194 pagesPack Alimentacion Clin in Perin 14Paz BustosNo ratings yet
- Micdak BackgroundDocument3 pagesMicdak Backgroundappiah ernestNo ratings yet
- Impact of Covid-19 On Audit Quality: Presented byDocument13 pagesImpact of Covid-19 On Audit Quality: Presented byMST. SADIYA SULTANANo ratings yet
- AYUSHMAN BHARAT Operationalizing Health and Wellness CentresDocument34 pagesAYUSHMAN BHARAT Operationalizing Health and Wellness CentresDr. Sachendra Raj100% (1)
- Fitness WalkingDocument192 pagesFitness Walkingjha.sofcon5941100% (1)
- BOF, LF & CasterDocument14 pagesBOF, LF & CastermaklesurrahmanNo ratings yet