You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chi Square TestDocument10 pagesChi Square Testarnav deshpandeNo ratings yet
- T-Tests Using Jamovi: By: Dr. Danny M. TeDocument15 pagesT-Tests Using Jamovi: By: Dr. Danny M. TeDarylNo ratings yet
- Pcba116 Module No. 7 Hypothesis TestingDocument18 pagesPcba116 Module No. 7 Hypothesis TestingSHARMAINE CORPUZ MIRANDANo ratings yet
- DATA ANALYSIS Result FileDocument5 pagesDATA ANALYSIS Result FileNuman RoxNo ratings yet
- Ward and Wilson 1978 PDFDocument13 pagesWard and Wilson 1978 PDFldv1452100% (1)
- Bus 308 Week 2 Problem Set Week TwoDocument11 pagesBus 308 Week 2 Problem Set Week Twoclaude_501486892No ratings yet
- T Test and ANOVA - Test: (Use Demo Discriptive - Sav Data File)Document5 pagesT Test and ANOVA - Test: (Use Demo Discriptive - Sav Data File)ishwaryaNo ratings yet
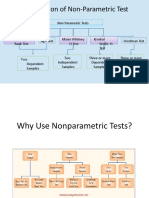
- Chapter 6 Non-Parametric and Robust TestDocument43 pagesChapter 6 Non-Parametric and Robust TestgirmaNo ratings yet
- Econ, Harv, MetricsDocument55 pagesEcon, Harv, Metricsscribewriter1990No ratings yet
- Analysis of Variance-1Document42 pagesAnalysis of Variance-1Varun BhayanaNo ratings yet
- Power Generation Systems (EL-321)Document7 pagesPower Generation Systems (EL-321)Habiba AzeemNo ratings yet
- BRM NotesDocument24 pagesBRM NotessuryaliNo ratings yet
- Stats Answer KeyDocument10 pagesStats Answer KeyJrlyn DaneNo ratings yet
- Research Question: A. Research Hypotheses What Is The Hypothesis?Document5 pagesResearch Question: A. Research Hypotheses What Is The Hypothesis?Byrence Aradanas BangsaliwNo ratings yet
- Hypothesis Testing For The Difference of ProportionsDocument6 pagesHypothesis Testing For The Difference of ProportionsAmarnathMaitiNo ratings yet
- Stress Level Between 3rd Year and 4th Year Nursing StudentfinalDocument5 pagesStress Level Between 3rd Year and 4th Year Nursing StudentfinalChristyl CalizoNo ratings yet
- Hypothesis Testing: Ervin C. ReyesDocument15 pagesHypothesis Testing: Ervin C. ReyesReyes C. ErvinNo ratings yet
- EngineeringDocument3 pagesEngineeringanand shrigondekarNo ratings yet
- Assessment.1 EXCEL MCQ Question BankDocument48 pagesAssessment.1 EXCEL MCQ Question Bankdibakardas10017No ratings yet
- Cyber Crime Project For MCOMDocument31 pagesCyber Crime Project For MCOMsachinNo ratings yet
- Black BookDocument12 pagesBlack BookSam ShaikhNo ratings yet
- MYLab 3Document4 pagesMYLab 3Mangala PrasetiaNo ratings yet
- Problem SetDocument6 pagesProblem SetKunal KumarNo ratings yet
- Guided-Discovery Learning Strategy and Senior School Students Performance in Mathematics in Ejigbo, NigeriaDocument9 pagesGuided-Discovery Learning Strategy and Senior School Students Performance in Mathematics in Ejigbo, NigeriaAlexander DeckerNo ratings yet
- Chapter 9: Introduction To The T StatisticDocument42 pagesChapter 9: Introduction To The T StatisticRhaine EstebanNo ratings yet
- Skew KurtosisDocument7 pagesSkew KurtosiscastjamNo ratings yet
- Gaps Silences and Comfort Zones Dominant Paradigms in Educational Drama and Applied Theatre DiscourseDocument17 pagesGaps Silences and Comfort Zones Dominant Paradigms in Educational Drama and Applied Theatre DiscourseSamantha AbelNo ratings yet
- STAB27Document51 pagesSTAB27Bharani DharanNo ratings yet
- Murray Sidman - Tactics of Scientific Research - Evaluating Experimental Data in PsychologyDocument442 pagesMurray Sidman - Tactics of Scientific Research - Evaluating Experimental Data in PsychologyHéctor Enrique Hernández HinojianteNo ratings yet
- Prerequisites, MFE Program, Berkeley-HaasDocument3 pagesPrerequisites, MFE Program, Berkeley-HaasAbynMathewScariaNo ratings yet