You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Afraid 1Document177 pagesAfraid 1Carvy DayritNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Culture of CebuDocument2 pagesCulture of CebuCarvy DayritNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Health Illness ContinuumDocument1 pageHealth Illness ContinuumCarvy DayritNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Quick Primer On Sampling TheoryDocument2 pagesA Quick Primer On Sampling TheoryCarvy DayritNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Antifungal DrugsDocument2 pagesAntifungal DrugsCarvy DayritNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
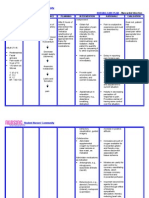
- Nursing Care Plan - Myocardial InfarctionDocument3 pagesNursing Care Plan - Myocardial Infarctionderic80% (10)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Nursing Care Plan HypertensionDocument2 pagesNursing Care Plan Hypertensionderic98% (124)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Ac CircuitsDocument2 pagesAc CircuitsCarvy DayritNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- PharmacologyDocument25 pagesPharmacologygregNo ratings yet
- Nle QuestionsDocument25 pagesNle QuestionsMhOt AmAd100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Living With Congestive Heart Failure CHF 4Document28 pagesLiving With Congestive Heart Failure CHF 4Soror RoseNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Ati Nclex NotesDocument10 pagesAti Nclex Notestipleton100% (4)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- DM M.CH - Curriculum For CardiologyDocument58 pagesDM M.CH - Curriculum For Cardiologyfindingnemo667No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- AnginaDocument43 pagesAnginaMuhammad Ashraf AhmadNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Pharmacology - A Summary of Common ConditionsDocument50 pagesPharmacology - A Summary of Common ConditionsJeremy YangNo ratings yet
- Cardiovascular DrugsDocument12 pagesCardiovascular DrugshannahcoNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Unstable Angina Differential DiagnosesDocument5 pagesUnstable Angina Differential DiagnosesSanda-ana BogdanNo ratings yet
- Nursing QuestionsDocument23 pagesNursing QuestionsTaSha Kalil MNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Smoking, Alcohol, and DrugsDocument13 pagesSmoking, Alcohol, and Drugs'Andi Mursyid Asrarsani'No ratings yet
- Eliminating Creatine Kinase-Myocardial Band Testing in Suspected Acute Coronary SyndromeDocument6 pagesEliminating Creatine Kinase-Myocardial Band Testing in Suspected Acute Coronary SyndromeRoberto López MataNo ratings yet
- Sample PrognosisDocument3 pagesSample PrognosisjudssalangsangNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medical Surgical Nursing Nclex QuestionsDocument82 pagesMedical Surgical Nursing Nclex Questionsdee_day_893% (14)
- 200 Hospital BenchmarksDocument16 pages200 Hospital BenchmarksMustafa BapaiNo ratings yet
- Drug StudyDocument11 pagesDrug StudyKimberly Subade MandilagNo ratings yet
- Medical Data Mining With Extended WEKA: R. ROBU and C. HORADocument4 pagesMedical Data Mining With Extended WEKA: R. ROBU and C. HORAShafayet UddinNo ratings yet
- Harvard Step Test: SkillslabDocument32 pagesHarvard Step Test: SkillslabRozman SepeaiNo ratings yet
- Pleural Effusion NCPsDocument7 pagesPleural Effusion NCPsJaja Nagallo100% (2)
- CBQ For NLEDocument10 pagesCBQ For NLEJerome VergaraNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Amls Als Pretest Version 1.11Document10 pagesAmls Als Pretest Version 1.11ArlanosaurusNo ratings yet
- Exercitii BoliDocument10 pagesExercitii BoliDanielaTanaseNo ratings yet
- Drug Study On Emergency DrugsDocument14 pagesDrug Study On Emergency DrugsRene John FranciscoNo ratings yet
- Nursing Board Review CardioDocument16 pagesNursing Board Review CardioPhilip Simangan100% (1)
- DrugsDocument7 pagesDrugsEloisa Abarintos RacalNo ratings yet
- High Yield NotesDocument211 pagesHigh Yield Notesroad2successNo ratings yet
- Drugs Affecting The Cardiovascular SystemDocument27 pagesDrugs Affecting The Cardiovascular SystemCelestino Kuchena100% (3)
- Acute Coronary Syndrome - A Case StudyDocument11 pagesAcute Coronary Syndrome - A Case StudyRocel Devilles100% (2)
- WRLD HRT DayDocument24 pagesWRLD HRT Daydas_s13No ratings yet
- AnginaDocument17 pagesAnginaGaming ModeNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)