You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Literary Portraiture & Modern Spain: Dr. Rebecca M. Bender (Document6 pagesLiterary Portraiture & Modern Spain: Dr. Rebecca M. Bender (Pedro PorbénNo ratings yet
- Index Medicus PDFDocument284 pagesIndex Medicus PDFVania Sitorus100% (1)
- AGIP STD - Valves Specification SheetDocument1 pageAGIP STD - Valves Specification Sheethalim_kaNo ratings yet
- Checklist For Surge Arrester Rev00Document3 pagesChecklist For Surge Arrester Rev00Santhosh Kumar VinayagamNo ratings yet
- Cyber Safety PP Presentation For Class 11Document16 pagesCyber Safety PP Presentation For Class 11WAZ CHANNEL100% (1)
- MCQ Homework: PeriodonticsDocument4 pagesMCQ Homework: Periodonticsفراس الموسويNo ratings yet
- Emission Estimation Technique Manual: For Mining and Processing of Non-Metallic MineralsDocument84 pagesEmission Estimation Technique Manual: For Mining and Processing of Non-Metallic MineralsAbdelaziem mahmoud abdelaalNo ratings yet
- Electric Field Summary NotesDocument11 pagesElectric Field Summary NotesVoyce Xavier PehNo ratings yet
- Team SportsDocument143 pagesTeam SportsYashNo ratings yet
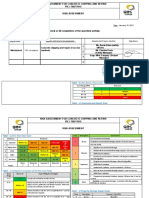
- Ra Concrete Chipping 7514Document5 pagesRa Concrete Chipping 7514Charles DoriaNo ratings yet
- RMP ContractDocument181 pagesRMP ContractHillary AmistosoNo ratings yet
- Hemostatic AgentsDocument18 pagesHemostatic AgentshariNo ratings yet
- Postoperative Care in Thoracic Surgery A Comprehensive GuideDocument397 pagesPostoperative Care in Thoracic Surgery A Comprehensive GuideΑΘΑΝΑΣΙΟΣ ΚΟΥΤΟΥΚΤΣΗΣ100% (1)
- Intentions and Results ASFA and Incarcerated ParentsDocument10 pagesIntentions and Results ASFA and Incarcerated Parentsaflee123No ratings yet
- Aakanksha ProjectDocument32 pagesAakanksha ProjectAakash murarkaNo ratings yet
- Uttarakhand District Factbook: Almora DistrictDocument33 pagesUttarakhand District Factbook: Almora DistrictDatanet IndiaNo ratings yet
- Careerride Com Electrical Engineering Interview Questions AsDocument21 pagesCareerride Com Electrical Engineering Interview Questions AsAbhayRajSinghNo ratings yet
- Essay 31 - Permissive ParentingDocument2 pagesEssay 31 - Permissive Parentingqbich37No ratings yet
- Constantino V MendezDocument3 pagesConstantino V MendezNīc CādīgālNo ratings yet
- Microsoft Security Intelligence Report Volume 21 EnglishDocument180 pagesMicrosoft Security Intelligence Report Volume 21 EnglishAlejandro CadarsoNo ratings yet
- Astm d2729Document2 pagesAstm d2729Shan AdriasNo ratings yet
- Case StudyDocument7 pagesCase StudyLeighvan PapasinNo ratings yet
- Chi - Square Test: PG Students: DR Amit Gujarathi DR Naresh GillDocument32 pagesChi - Square Test: PG Students: DR Amit Gujarathi DR Naresh GillNaresh GillNo ratings yet
- Pressure Vessels SHO ProgrammeDocument42 pagesPressure Vessels SHO Programmehew ka yeeNo ratings yet
- Action Taken On Oil and Ghee Sampling - 2020Document2 pagesAction Taken On Oil and Ghee Sampling - 2020Khalil BhattiNo ratings yet
- 21A Solenoid Valves Series DatasheetDocument40 pages21A Solenoid Valves Series Datasheetportusan2000No ratings yet
- ომარ ხაიამი - რობაიები (პარალელური ტექსტები)Document31 pagesომარ ხაიამი - რობაიები (პარალელური ტექსტები)გენო მუმლაძეNo ratings yet
- f2607-#### f2607 20191203 111644Document2 pagesf2607-#### f2607 20191203 111644คุณชายธวัชชัย เจริญสุขNo ratings yet
- 3 Ways To Take Isabgol - WikiHowDocument6 pages3 Ways To Take Isabgol - WikiHownasirNo ratings yet