You might also like
- Disease of Prostate Tutorial-Dec-2014Document49 pagesDisease of Prostate Tutorial-Dec-2014marina_shawkyNo ratings yet
- Night Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNight Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Swollen Kidney, (Hydronephrosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSwollen Kidney, (Hydronephrosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Disseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDisseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Desmoid Tumor2-1Document29 pagesDesmoid Tumor2-1basmarizk deabsNo ratings yet
- 18 - Flow Cytometry and Introduction To Molecular PathologyDocument11 pages18 - Flow Cytometry and Introduction To Molecular Pathologyhamadadodo7No ratings yet
- Nephrotic and Nephritic Syndrome - 2008Document65 pagesNephrotic and Nephritic Syndrome - 2008rikasusanti101001201No ratings yet
- Blood TransfusionDocument23 pagesBlood TransfusionMohammad Husni Banisalman100% (1)
- Graft RejectionDocument33 pagesGraft Rejectionasmaa100% (1)
- Lecture On Anemias and Polycythemias by Dr. RoomiDocument30 pagesLecture On Anemias and Polycythemias by Dr. RoomiMudassar Roomi100% (1)
- Blood Investigations: Dr. Maulika PatelDocument21 pagesBlood Investigations: Dr. Maulika Patelpatrikmodi100% (1)
- Term Paper ON: Correlation Between Rapid Test and Automated Methods in Diagnosing Infectious Disease Like TyphoidDocument22 pagesTerm Paper ON: Correlation Between Rapid Test and Automated Methods in Diagnosing Infectious Disease Like TyphoidSoniya DhyaniNo ratings yet
- GALACTOSEMIAlabDocument49 pagesGALACTOSEMIAlabShen VillamilNo ratings yet
- What Should Not You Do in A Research?Document27 pagesWhat Should Not You Do in A Research?Mohd HardyNo ratings yet
- MNT in Diseases of Kidney and UrinaryDocument38 pagesMNT in Diseases of Kidney and UrinaryJosephine A. Bertulfo100% (1)
- Blood Transfusion PDFDocument20 pagesBlood Transfusion PDFalaamorsyNo ratings yet
- Renal Replacement Therapy HD, PD, Renal TransplantationDocument65 pagesRenal Replacement Therapy HD, PD, Renal TransplantationparciNo ratings yet
- Endocrine Pathology LectureDocument31 pagesEndocrine Pathology Lectureninja2007No ratings yet
- CanserDocument50 pagesCansertarek ahmed100% (1)
- Faquin Milian System and Molecular Advances in Diagnosis Salivary Gland TumorsDocument87 pagesFaquin Milian System and Molecular Advances in Diagnosis Salivary Gland TumorsJoanna Marie100% (1)
- Tumours of The Central Nervous System: FM Brett MD., FrcpathDocument57 pagesTumours of The Central Nervous System: FM Brett MD., FrcpathDrGasnasNo ratings yet
- Renal Transplant: 1) Steps Involved in Kidney TransplantationDocument4 pagesRenal Transplant: 1) Steps Involved in Kidney TransplantationNadia SalwaniNo ratings yet
- LESSON 9 Organ Donation ActDocument56 pagesLESSON 9 Organ Donation ActnullNo ratings yet
- Thyroid NodulesDocument34 pagesThyroid NodulesEphobiaNo ratings yet
- Organ DonationDocument9 pagesOrgan DonationAravindan Sundar100% (1)
- BCLSDocument25 pagesBCLSikram ullah khanNo ratings yet
- Neuroblastoma My Lecture 2011Document153 pagesNeuroblastoma My Lecture 2011Wael ElsawyNo ratings yet
- PPTDocument61 pagesPPTHendra Devandra100% (1)
- REPORTING CERVICAL CYTOLOGY, The Bethesda SystemDocument3 pagesREPORTING CERVICAL CYTOLOGY, The Bethesda SystemNgotelo FunwiNo ratings yet
- A Brief Look at Renal AnatomyDocument15 pagesA Brief Look at Renal AnatomyKristina De Peralta Willy100% (1)
- Prostate and Seminal VesiclesDocument83 pagesProstate and Seminal Vesiclesgreg_enricoNo ratings yet
- Urethral Urinary CatheterizationDocument22 pagesUrethral Urinary CatheterizationXU Council of Nursing StudentsNo ratings yet
- Anatomy of The KidneysDocument7 pagesAnatomy of The KidneysSanthu SuNo ratings yet
- Micro Biology: Pgei Golden Points 2015Document27 pagesMicro Biology: Pgei Golden Points 2015Challa Krishna VasanNo ratings yet
- Chronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDocument42 pagesChronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDon RaulNo ratings yet
- Renal Abscess, Xanthogranulomatous Pyelonephritis and Renal TuberculosisDocument41 pagesRenal Abscess, Xanthogranulomatous Pyelonephritis and Renal TuberculosisAnas Mk HindawiNo ratings yet
- Kidney Function TestDocument19 pagesKidney Function Testbeena gracelyn sarahNo ratings yet
- Genitourinary: Drafnan Abdirahman MohamedDocument163 pagesGenitourinary: Drafnan Abdirahman MohamedMuse MuseNo ratings yet
- Hema II Chapter 7 - BM ExaminationDocument42 pagesHema II Chapter 7 - BM ExaminationKeerthy VasanNo ratings yet
- Liver Function TestDocument20 pagesLiver Function TestAvi VermaNo ratings yet
- Urine AnalysisDocument63 pagesUrine AnalysisVench DemicaisNo ratings yet
- Lymphoma: Pro - Dr.Ahmed EisaDocument45 pagesLymphoma: Pro - Dr.Ahmed EisaOmar Mohammed100% (1)
- Haemorrhage & Blood TransfusionDocument60 pagesHaemorrhage & Blood TransfusionSehar162100% (2)
- Specimen Collection, Transport and ProcessingDocument29 pagesSpecimen Collection, Transport and ProcessingGladys Marie WillkomNo ratings yet
- Neoplasia 2011 ADocument45 pagesNeoplasia 2011 ACassey Koi FarmNo ratings yet
- Urolithiasis: ObjectivesDocument11 pagesUrolithiasis: ObjectivesOkki Masitah Syahfitri NasutionNo ratings yet
- Orientation To Blood Bank 2Document24 pagesOrientation To Blood Bank 2Darshita SharmaNo ratings yet
- Urinary Tract CalculiDocument34 pagesUrinary Tract CalculiOnkar SinghNo ratings yet
- Rayneilda Eleana Siew MLT U29 Unit Makmal Patologi Hospital Nukleus WP LabuanDocument17 pagesRayneilda Eleana Siew MLT U29 Unit Makmal Patologi Hospital Nukleus WP LabuanValentine Brokenz Saintz100% (1)
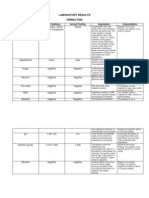
- Laboratory ResultsDocument4 pagesLaboratory ResultsRoxanne Ganayo ClaverNo ratings yet
- Chronic CholecystitisDocument7 pagesChronic CholecystitisErika alfonsoNo ratings yet
- Cerebral EdemaDocument21 pagesCerebral EdemasridharNo ratings yet
- How Does Haemodialysis WorkDocument19 pagesHow Does Haemodialysis Workhello_khay100% (1)
- Suprarenal (Adrenal) Gland: Dr. R. SanthakumarDocument33 pagesSuprarenal (Adrenal) Gland: Dr. R. SanthakumardrsubanNo ratings yet
- James Griffiths Consultant em Barnsley Cem Foamed Network: @yorkshumberfoamDocument17 pagesJames Griffiths Consultant em Barnsley Cem Foamed Network: @yorkshumberfoamDede MaulanaNo ratings yet
- Prevention of DVT/PE: Noornadia BT Yahaya 050100841Document32 pagesPrevention of DVT/PE: Noornadia BT Yahaya 050100841Nadia YahayaNo ratings yet
- Pituitary Tumors Engleza 2Document89 pagesPituitary Tumors Engleza 2Achmad Harun MuchsinNo ratings yet
- Thymoma: Rawa MuhsinDocument53 pagesThymoma: Rawa MuhsinRawa MuhsinNo ratings yet
- Grossing Uterus Presentation1Document19 pagesGrossing Uterus Presentation1jayesh saha100% (1)
- Urine Incontinence Care: Urine Catheters Urine Bags AccessoriesDocument24 pagesUrine Incontinence Care: Urine Catheters Urine Bags AccessoriesMerveNo ratings yet
- Spinal Cord Injury Guide AssessmentDocument11 pagesSpinal Cord Injury Guide AssessmentKingsley Martinez CastroNo ratings yet
- November 2008 NLE Practice IVDocument19 pagesNovember 2008 NLE Practice IVEJ Cubero, R☤NNo ratings yet
- VUMC Urinary Catheter GuidelinesDocument5 pagesVUMC Urinary Catheter GuidelinesNurul UswatinNo ratings yet
- Checklist of Quality Indicators For NABH Accreditation PreparationDocument11 pagesChecklist of Quality Indicators For NABH Accreditation PreparationQUALITY SIDARTH HOSPITALSNo ratings yet
- 7 PsccauticurrentDocument22 pages7 PsccauticurrentLuz Glenny CastroNo ratings yet
- Basic Ward ProceduresDocument209 pagesBasic Ward ProceduresNoopur SawarkarNo ratings yet
- Seminar On Infetion ControlDocument76 pagesSeminar On Infetion ControlDaisy Vinu0% (1)
- Male Female Catheterization Rle 30Document95 pagesMale Female Catheterization Rle 30HoneylouAzOpondaNo ratings yet
- Standard Treatment: Guidelines 2022Document6 pagesStandard Treatment: Guidelines 2022Swathi KrishnaNo ratings yet
- Research QuestionnaireDocument3 pagesResearch QuestionnaireJason Roy Edward NathanNo ratings yet
- DR Instrument (Recovered)Document25 pagesDR Instrument (Recovered)Mayolianne DumayNo ratings yet
- Laparoscopic CholecystectomyDocument10 pagesLaparoscopic CholecystectomyCharm TanyaNo ratings yet
- Revised CATHETERIZATION 2Document43 pagesRevised CATHETERIZATION 2Insatiable CleeNo ratings yet
- Bladder Training (For Resident With A Catheter)Document2 pagesBladder Training (For Resident With A Catheter)Charley Degamo100% (1)
- EliminationDocument128 pagesEliminationhailye mitikeNo ratings yet
- Copy (3) of Urinary CatheterizationDocument21 pagesCopy (3) of Urinary CatheterizationAbogadie Dione Blas ReyNo ratings yet
- Spina Bifida: A Guide For School Personnel Working With Students WithDocument37 pagesSpina Bifida: A Guide For School Personnel Working With Students WithGuz CaemmNo ratings yet
- Infeksi Bakteri Pada Traktus Urinarius-2015Document55 pagesInfeksi Bakteri Pada Traktus Urinarius-2015fuad20No ratings yet
- Browning V Burt, 66 Ohio St.3d 544 (Ohio 1993)Document60 pagesBrowning V Burt, 66 Ohio St.3d 544 (Ohio 1993)magis00No ratings yet
- Bladder Catheterisation PDFDocument12 pagesBladder Catheterisation PDFSonish KhatriNo ratings yet
- Ultrazvuk AbdomenaDocument10 pagesUltrazvuk AbdomenaLejlaNo ratings yet
- Catheter-Associated Urinary Tract Infection Care BundleDocument3 pagesCatheter-Associated Urinary Tract Infection Care BundleAnisaNo ratings yet
- Specimen CollectionDocument10 pagesSpecimen CollectionjaljimNo ratings yet
- Chronic Complications of Spinal Cord Injury and Disease - UpToDateDocument25 pagesChronic Complications of Spinal Cord Injury and Disease - UpToDateElinaldo Soares Costa SilvaNo ratings yet
- Bladder StonesDocument20 pagesBladder StonesRiean AuliaNo ratings yet
- Romsons All ProductDocument53 pagesRomsons All ProductBoyke WinterbergNo ratings yet
- Urinary RetentionDocument6 pagesUrinary Retentionjakenathanielvelasco50% (2)
- Dar Shahid Yousuf, 361, EpidemiologyDocument36 pagesDar Shahid Yousuf, 361, EpidemiologyShahid Yousuf DarNo ratings yet
- Cath PlanDocument1 pageCath PlanJade Ann LorezoNo ratings yet