You might also like
- It's Not Just a Heavy Period; The Miscarriage HandbookFrom EverandIt's Not Just a Heavy Period; The Miscarriage HandbookRating: 2 out of 5 stars2/5 (1)
- Antepartum HemorrhageDocument26 pagesAntepartum Hemorrhageariani putri devantiNo ratings yet
- Ectopic Pregnancy BWDocument28 pagesEctopic Pregnancy BWZiya AkhtarNo ratings yet
- Antepartum HemorrhageDocument18 pagesAntepartum HemorrhageSanaNo ratings yet
- Placenta Previa and Abruptio Placenta: Presenter Eessaa ShresthaDocument72 pagesPlacenta Previa and Abruptio Placenta: Presenter Eessaa ShresthaEsa SthaNo ratings yet
- Antepartum HemorrhageDocument43 pagesAntepartum HemorrhageashwiniNo ratings yet
- Antepartum Haemorrhage (APH) : DR Nitin TiwariDocument49 pagesAntepartum Haemorrhage (APH) : DR Nitin TiwariPravin SasaneNo ratings yet
- BaruCH03 Obst HaemorrhageDocument57 pagesBaruCH03 Obst Haemorrhagenot_a_geekNo ratings yet
- Antepartum HaemorrhageDocument25 pagesAntepartum HaemorrhagesyedsuhailalishahNo ratings yet
- Early Pregnancy CareDocument42 pagesEarly Pregnancy Caremiloja.simpsonNo ratings yet
- APH DR DaudDocument56 pagesAPH DR DaudMohd Daud Che YusofNo ratings yet
- Antepartum Haemorrhage Guidelines For The Management of - ABMU Guideline 201Document5 pagesAntepartum Haemorrhage Guidelines For The Management of - ABMU Guideline 201ubayyumrNo ratings yet
- Antepartum HemorrhageDocument48 pagesAntepartum HemorrhageJoshua EvansNo ratings yet
- Antepartum HeamorrhageDocument34 pagesAntepartum HeamorrhageSHOWMAN DEEPAKNo ratings yet
- OB Intern's Review - Dra LeeDocument214 pagesOB Intern's Review - Dra LeeKathleenZunigaNo ratings yet
- Placenta Previa MarginalDocument51 pagesPlacenta Previa MarginalMedy WedhanggaNo ratings yet
- Asuhan Keperawatan Kegawatdaruratan Maternal Pada Kasus Ket: Maria Lupita Nena MeoDocument20 pagesAsuhan Keperawatan Kegawatdaruratan Maternal Pada Kasus Ket: Maria Lupita Nena MeoCathleen GunawanNo ratings yet
- Ectopic PregnancyDocument20 pagesEctopic PregnancyCathleen GunawanNo ratings yet
- First Trimester Bleeding: Bagian Obstetri Dan Ginekologi Fakultas Kedokteran Universitas Diponegoro Semarang 2016Document65 pagesFirst Trimester Bleeding: Bagian Obstetri Dan Ginekologi Fakultas Kedokteran Universitas Diponegoro Semarang 2016Peggy SyahputraNo ratings yet
- Objectives of Aph:: To Define About APH. To List The Causes of APHDocument42 pagesObjectives of Aph:: To Define About APH. To List The Causes of APHReena TyagiNo ratings yet
- Antepartum BleedingDocument55 pagesAntepartum BleedingMunfaati AbdiyahNo ratings yet
- Perdarahan AntepartumDocument52 pagesPerdarahan AntepartumFaiqah AzahraNo ratings yet
- Miscarriage Early Pregnancy LossDocument10 pagesMiscarriage Early Pregnancy LossiwennieNo ratings yet
- Management of Obstetric HaemorrhageDocument89 pagesManagement of Obstetric HaemorrhageMohammad AlrefaiNo ratings yet
- Bleeding in Early Late PregnancyDocument46 pagesBleeding in Early Late PregnancyAndrada Catrinoiu100% (2)
- Antepartum HaemorrhageDocument49 pagesAntepartum Haemorrhagereshma somarajanNo ratings yet
- Antepartum HaemorhageDocument31 pagesAntepartum HaemorhageOoi Say TingNo ratings yet
- Third Trimester Bleeding 12Document34 pagesThird Trimester Bleeding 12rayankemo31No ratings yet
- Complications During Pregnancy - Chapt 5 - 1Document40 pagesComplications During Pregnancy - Chapt 5 - 1Bob IrsanNo ratings yet
- MLC Interns Review 2011 - Dra ColomaDocument251 pagesMLC Interns Review 2011 - Dra ColomaKathleenZunigaNo ratings yet
- Antepartum HaemorrhageDocument32 pagesAntepartum HaemorrhageRyaa Nitaa AdyaaNo ratings yet
- Antepartum & Postpartum Hemorrhage (APH &PPH) : Basim Abu-RafeaDocument81 pagesAntepartum & Postpartum Hemorrhage (APH &PPH) : Basim Abu-RafeaSheilla ElfiraNo ratings yet
- Approach To EPBDocument30 pagesApproach To EPBMahmoud Abu Al AmrainNo ratings yet
- Abruptio Placenta For StudentsDocument26 pagesAbruptio Placenta For Studentssonam MaclayNo ratings yet
- Ectopic PregnancyDocument32 pagesEctopic Pregnancyyt2zkpkphqNo ratings yet
- Ectopic Pregnancy ADocument37 pagesEctopic Pregnancy AJervhen Sky Adolfo Dalisan100% (1)
- Prenatal ScreeningDocument61 pagesPrenatal Screeningjoycechicago100% (1)
- Obstetrical HemorrhageDocument76 pagesObstetrical HemorrhagejarssooNo ratings yet
- Placenta Previa MarginalDocument50 pagesPlacenta Previa MarginalMedy WedhanggaNo ratings yet
- Antepartum HemorrhageDocument81 pagesAntepartum HemorrhageOmar mohamedNo ratings yet
- High Risk Conditions During Labor and DeliveryDocument14 pagesHigh Risk Conditions During Labor and DeliveryEdgar HinotanNo ratings yet
- Identifying Clients at RiskDocument57 pagesIdentifying Clients at Riskcoosa liquors100% (1)
- Placenta Previa: Supervised By: Dr. Pim Gonta, SP - OGDocument24 pagesPlacenta Previa: Supervised By: Dr. Pim Gonta, SP - OGPrincella MonicaNo ratings yet
- Antepartum Haemorrhage (APH) : Prepared by Helen CookeDocument22 pagesAntepartum Haemorrhage (APH) : Prepared by Helen CookejojolilimomoNo ratings yet
- Obstetric Highlights Elmar P. Sakala PDFDocument47 pagesObstetric Highlights Elmar P. Sakala PDFwalt65No ratings yet
- Seminar 11 APH and PPHDocument61 pagesSeminar 11 APH and PPHIshak IzharNo ratings yet
- Antepartum Haemorrhage MXDocument22 pagesAntepartum Haemorrhage MXAmir Hilmi Abd AzizNo ratings yet
- 2 Pre Gestation and Gestational ConditionsDocument88 pages2 Pre Gestation and Gestational Conditionslermacornel61No ratings yet
- What The Bleep?: Common Calls For Junior Doctors in O&G DR Alice KnowlesDocument43 pagesWhat The Bleep?: Common Calls For Junior Doctors in O&G DR Alice KnowlesAlice KnowlesNo ratings yet
- Antepartum HemorrhageDocument52 pagesAntepartum HemorrhageKomalah ChenasammyNo ratings yet
- Bleeding in Early and Late: PregnancyDocument31 pagesBleeding in Early and Late: Pregnancysny007No ratings yet
- NCM 209 Lesson 1 FinallDocument8 pagesNCM 209 Lesson 1 Finalldanica grace gubaNo ratings yet
- Placenta PreviaDocument12 pagesPlacenta Previapatriciagchiu100% (3)
- Antepartum BleedingDocument37 pagesAntepartum BleedingMae Importers IncNo ratings yet
- Maternity Nursing Review: Ahmed El KahloutDocument60 pagesMaternity Nursing Review: Ahmed El KahloutHabebt MusabNo ratings yet
- Abruptio PlacentaDocument36 pagesAbruptio PlacentaBriandon CanlasNo ratings yet
- PACES Revision Obstetrics and Gynaecology: 27/04/2012 Amrita Banerjee & Ola MarkiewiczDocument62 pagesPACES Revision Obstetrics and Gynaecology: 27/04/2012 Amrita Banerjee & Ola MarkiewiczThistell ThistleNo ratings yet
- Placenta Abruptio: Maneja, Jan Michael B. BSN 223Document6 pagesPlacenta Abruptio: Maneja, Jan Michael B. BSN 223JiraGonzales100% (1)
- OB/GYN For EMS ProvidersDocument94 pagesOB/GYN For EMS ProvidersPaulhotvw67100% (6)
- Early Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelDocument60 pagesEarly Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelmedicoNo ratings yet
- CataractDocument3 pagesCataractSetiawan Arif WibowoNo ratings yet
- Early Vs Late Traumatic CataractDocument6 pagesEarly Vs Late Traumatic CataractSetiawan Arif WibowoNo ratings yet
- Papillitis DeleonjodyDocument2 pagesPapillitis DeleonjodySetiawan Arif WibowoNo ratings yet
- NIH Public Access: The Pathophysiology of Thyroid Eye Disease (TED) : Implications For ImmunotherapyDocument10 pagesNIH Public Access: The Pathophysiology of Thyroid Eye Disease (TED) : Implications For ImmunotherapySetiawan Arif WibowoNo ratings yet
- 31 McMahon - A New Method Keratoconus PDFDocument7 pages31 McMahon - A New Method Keratoconus PDFSetiawan Arif WibowoNo ratings yet
- Amsler Grid PDFDocument1 pageAmsler Grid PDFSetiawan Arif WibowoNo ratings yet
- CanaliculitisDocument12 pagesCanaliculitisSetiawan Arif WibowoNo ratings yet
- Cotton Combed Round Neck 20's (Satuan) Ukuran Putih Hitam Warna LainDocument2 pagesCotton Combed Round Neck 20's (Satuan) Ukuran Putih Hitam Warna LainSetiawan Arif WibowoNo ratings yet
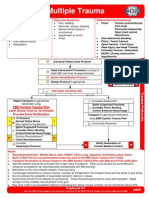
- Multiple Trauma EvaluationDocument2 pagesMultiple Trauma EvaluationSetiawan Arif WibowoNo ratings yet
- Selulitis PDFDocument5 pagesSelulitis PDFDhisa Zainita HabsariNo ratings yet
- 1 s2.0 S0146000515001962Document14 pages1 s2.0 S0146000515001962Setiawan Arif WibowoNo ratings yet
- Paediatrics and Child Health Volume 22 Issue 1 2012 (Doi 10.1016 - J.paed.2011.04.002) Patrick Watts - Preseptal and Orbital Cellulitis in Children - A ReviewDocument8 pagesPaediatrics and Child Health Volume 22 Issue 1 2012 (Doi 10.1016 - J.paed.2011.04.002) Patrick Watts - Preseptal and Orbital Cellulitis in Children - A ReviewSetiawan Arif WibowoNo ratings yet
- Mayoclinic Management SEDocument11 pagesMayoclinic Management SESetiawan Arif WibowoNo ratings yet
- Critical Appraisal of The International Subarachnoid Aneurysm Trial (ISAT)Document7 pagesCritical Appraisal of The International Subarachnoid Aneurysm Trial (ISAT)Setiawan Arif WibowoNo ratings yet
- Multiple Trauma ManagementDocument1 pageMultiple Trauma ManagementSetiawan Arif WibowoNo ratings yet
- Publications Safe AbortionDocument110 pagesPublications Safe AbortionSetiawan Arif WibowoNo ratings yet
- Episiotomy RcogDocument1 pageEpisiotomy RcogAisha RizwanNo ratings yet
- CREO Objetivos ACOGDocument48 pagesCREO Objetivos ACOGMiguel Gómez100% (1)
- Presentation BreastDocument17 pagesPresentation Breastmayeth galeraNo ratings yet
- Aim4aiims - In: 30-GynecologyDocument13 pagesAim4aiims - In: 30-GynecologyAnwaar YousafNo ratings yet
- Detailed Record of CPD Activities Name: Ooi Siew Thin IC NO:620423-02-5398 Position/Gred: Jururawat 42 From (Month/Year) : August 2018 To 2019Document2 pagesDetailed Record of CPD Activities Name: Ooi Siew Thin IC NO:620423-02-5398 Position/Gred: Jururawat 42 From (Month/Year) : August 2018 To 2019MrS DNo ratings yet
- Assessment of Maternal Knowledge, Attitudes, and Practices Regarding Breastfeeding at Kampala International Teaching Hospital A Study Spanning May 2021 To July 2022Document15 pagesAssessment of Maternal Knowledge, Attitudes, and Practices Regarding Breastfeeding at Kampala International Teaching Hospital A Study Spanning May 2021 To July 2022KIU PUBLICATION AND EXTENSIONNo ratings yet
- Menstrual Cycle LP - 1st CODocument8 pagesMenstrual Cycle LP - 1st COEsther Mae Ann TrugilloNo ratings yet
- Mark Fredderick R. Abejo RN, MAN: Maternal and Child Nursing BulletsDocument9 pagesMark Fredderick R. Abejo RN, MAN: Maternal and Child Nursing BulletsCrystal Ann Monsale TadiamonNo ratings yet
- Untitled28 PDFDocument14 pagesUntitled28 PDFElizabeth Leon100% (1)
- Molar PregnancyDocument5 pagesMolar Pregnancycwqdtgtf6hNo ratings yet
- Retained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateDocument19 pagesRetained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateHartanto Lie100% (1)
- Lactational Amenorrhea: Sumita Shakya Sushila Gautam Tila Sharma B.SC Nursing (2017)Document16 pagesLactational Amenorrhea: Sumita Shakya Sushila Gautam Tila Sharma B.SC Nursing (2017)Sunita GurungNo ratings yet
- Askeb Terapi Daun KubisDocument8 pagesAskeb Terapi Daun KubisArryaniNo ratings yet
- UntitledDocument8 pagesUntitledPJ Manuel SuerteNo ratings yet
- Nursing Care During PregnancyDocument41 pagesNursing Care During PregnancyEvan ChrissantaNo ratings yet
- L P APHDocument11 pagesL P APHmoni khatkarNo ratings yet
- Reproductive Cycles in MammalsDocument9 pagesReproductive Cycles in MammalsSeemal shahidNo ratings yet
- Placental Abruption PresentationDocument30 pagesPlacental Abruption PresentationNafisat AdepojuNo ratings yet
- Dra Juson Labor & DeliveryDocument153 pagesDra Juson Labor & DeliveryaringkinkingNo ratings yet
- Diagnostic Tests For Female InfertilityDocument4 pagesDiagnostic Tests For Female InfertilityFalensia Dwita LestariNo ratings yet
- Mode of Delivery and Persistence of Pelvic Girdle Syndrome 6 Months PostpartumDocument20 pagesMode of Delivery and Persistence of Pelvic Girdle Syndrome 6 Months PostpartumDanil ArmandNo ratings yet
- Incomplete AbortionDocument4 pagesIncomplete AbortionAira Jane MuñozNo ratings yet
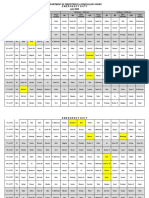
- Department of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020Document3 pagesDepartment of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020noorNo ratings yet
- Family Planning MethodDocument22 pagesFamily Planning MethodPrince XianderNo ratings yet
- AUBDocument10 pagesAUBFathy ElsheshtawyNo ratings yet
- DR Fleischer Obstetric Hemorrhage PresentationDocument66 pagesDR Fleischer Obstetric Hemorrhage PresentationHabebt MusabNo ratings yet
- Puerperal Sepsis PDFDocument10 pagesPuerperal Sepsis PDFtanmai nooluNo ratings yet
- M Vanguardia-McnpDocument11 pagesM Vanguardia-Mcnpmark OrpillaNo ratings yet
- Case On InfertilityDocument26 pagesCase On InfertilityGazala ParveenNo ratings yet
- Labour and Delivery Nursing CareDocument40 pagesLabour and Delivery Nursing CareNica Baldedara100% (3)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayFrom EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayRating: 4.5 out of 5 stars4.5/5 (3)
- What to Expect When You’re Expecting (5th Edition)From EverandWhat to Expect When You’re Expecting (5th Edition)Rating: 5 out of 5 stars5/5 (1)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeFrom EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeRating: 3.5 out of 5 stars3.5/5 (13)
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeFrom EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeNo ratings yet
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouFrom EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo ratings yet
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodFrom EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodRating: 5 out of 5 stars5/5 (33)
- A Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersFrom EverandA Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersRating: 4.5 out of 5 stars4.5/5 (71)
- Spirit Baby: Communicate with Your Unborn Baby. Ease Your BirthFrom EverandSpirit Baby: Communicate with Your Unborn Baby. Ease Your BirthRating: 5 out of 5 stars5/5 (1)
- Awakening Fertility: The Essential Art of Preparing for PregnancyFrom EverandAwakening Fertility: The Essential Art of Preparing for PregnancyRating: 4.5 out of 5 stars4.5/5 (36)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondFrom EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondRating: 4.5 out of 5 stars4.5/5 (38)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.From EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Rating: 4.5 out of 5 stars4.5/5 (124)
- The Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityFrom EverandThe Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityRating: 4.5 out of 5 stars4.5/5 (12)
- ADHD Women: A Holistic Approach To ADHD ManagementFrom EverandADHD Women: A Holistic Approach To ADHD ManagementRating: 5 out of 5 stars5/5 (4)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenFrom EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenRating: 4 out of 5 stars4/5 (154)
- Labor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodFrom EverandLabor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodRating: 4.5 out of 5 stars4.5/5 (28)
- Women, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainFrom EverandWomen, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainRating: 4 out of 5 stars4/5 (14)
- Medical Bondage: Race, Gender, and the Origins of American GynecologyFrom EverandMedical Bondage: Race, Gender, and the Origins of American GynecologyRating: 4.5 out of 5 stars4.5/5 (75)
- I'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionFrom EverandI'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionRating: 4.5 out of 5 stars4.5/5 (125)
- Crones Don't Whine: Concentrated Wisdom for Juicy WomenFrom EverandCrones Don't Whine: Concentrated Wisdom for Juicy WomenRating: 2.5 out of 5 stars2.5/5 (3)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondFrom EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondRating: 4.5 out of 5 stars4.5/5 (3)
- Pregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!From EverandPregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!Rating: 5 out of 5 stars5/5 (1)
- Awakening Fertility: The Essential Art of Preparing for PregnancyFrom EverandAwakening Fertility: The Essential Art of Preparing for PregnancyRating: 5 out of 5 stars5/5 (4)
- Mindful Birthing: Training the Mind, Body, and Heart for Childbirth and BeyondFrom EverandMindful Birthing: Training the Mind, Body, and Heart for Childbirth and BeyondRating: 4 out of 5 stars4/5 (15)
- The Strength and Conditioning Bible: How to Train Like an AthleteFrom EverandThe Strength and Conditioning Bible: How to Train Like an AthleteNo ratings yet
- Younger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondFrom EverandYounger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondRating: 4 out of 5 stars4/5 (111)
- I'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionFrom EverandI'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionRating: 4 out of 5 stars4/5 (27)
- Eat To Live Diet: The Ultimate Step by Step Cheat Sheet on How To Lose Weight & Sustain It NowFrom EverandEat To Live Diet: The Ultimate Step by Step Cheat Sheet on How To Lose Weight & Sustain It NowRating: 3 out of 5 stars3/5 (3)
- What No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodFrom EverandWhat No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodRating: 4.5 out of 5 stars4.5/5 (30)