You might also like
- 1Document4 pages1Dashari Ermandi HNo ratings yet
- LK September 2019Document1 pageLK September 2019Dashari Ermandi HNo ratings yet
- Foto FotoDocument7 pagesFoto FotoDashari Ermandi HNo ratings yet
- Jadwal BHD RSKM SeptemberDocument3 pagesJadwal BHD RSKM SeptemberDashari Ermandi HNo ratings yet
- Berita Acara April 2019Document1 pageBerita Acara April 2019Dashari Ermandi HNo ratings yet
- Absen Operasional 2019Document6 pagesAbsen Operasional 2019Dashari Ermandi HNo ratings yet
- Absen Operasional SeptemberDocument10 pagesAbsen Operasional SeptemberDashari Ermandi HNo ratings yet
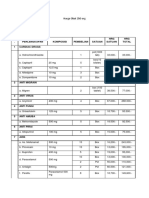
- Harga Obat 250 OrgDocument5 pagesHarga Obat 250 OrgDashari Ermandi HNo ratings yet
- Abscess Evaluation Using Bedside UltrasonographyDocument8 pagesAbscess Evaluation Using Bedside UltrasonographyDashari Ermandi HNo ratings yet
- Harga Obat 250 OrgDocument5 pagesHarga Obat 250 OrgDashari Ermandi HNo ratings yet
- Harga Obat 250 OrgDocument5 pagesHarga Obat 250 OrgDashari Ermandi HNo ratings yet
- Nicemedia LiveDocument57 pagesNicemedia LiveLawrence McleodNo ratings yet
- Follow Up: Tanggal 18-21 Mei 2014 S: Demam (-), Nyeri Pinggang (-) O: TD: 110/70 MMHGDocument2 pagesFollow Up: Tanggal 18-21 Mei 2014 S: Demam (-), Nyeri Pinggang (-) O: TD: 110/70 MMHGDashari Ermandi HNo ratings yet
- Acute Coronary SyndromeDocument45 pagesAcute Coronary SyndromeDashari Ermandi HNo ratings yet
- Benign Conditions of The Thyroid Gland Just SeeDocument5 pagesBenign Conditions of The Thyroid Gland Just SeeDashari Ermandi HNo ratings yet
- K24 Baru Kuliah Malaria Blok TropmedDocument17 pagesK24 Baru Kuliah Malaria Blok TropmedDashari Ermandi HNo ratings yet
- Lampiran IraDocument3 pagesLampiran IraDashari Ermandi HNo ratings yet
- Format Penilaian PelatihanDocument2 pagesFormat Penilaian PelatihanDashari Ermandi HNo ratings yet
- Cannulation 1Document5 pagesCannulation 1TONY GO AWAYNo ratings yet
- Hipertensi 1Document7 pagesHipertensi 1Dashari Ermandi HNo ratings yet
- K 2 - PBLDocument18 pagesK 2 - PBLDashari Ermandi HNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Functional Neuroanatomy of The Basal Ganglia (Lanciego, Luquin & Obeso, 2012)Document21 pagesFunctional Neuroanatomy of The Basal Ganglia (Lanciego, Luquin & Obeso, 2012)Rocío Donaire CortésNo ratings yet
- Dopamin 2 PDFDocument8 pagesDopamin 2 PDFdonkeyendutNo ratings yet
- Basal GangliaDocument32 pagesBasal GangliaManisanthosh Kumar100% (2)
- Krieshok2009 PDFDocument16 pagesKrieshok2009 PDFAlexandru NaeNo ratings yet
- Sistem Syaraf Manusia: Nanda Fadhilah Witris Salamy, DRDocument15 pagesSistem Syaraf Manusia: Nanda Fadhilah Witris Salamy, DRwitrisalamyNo ratings yet
- Anatomía funcional de los ganglios basalesDocument6 pagesAnatomía funcional de los ganglios basalesIván DelgadoNo ratings yet
- Rat Brain AtlasDocument463 pagesRat Brain AtlasRezidens Neurológus100% (3)
- WeyandtDocument408 pagesWeyandtAntonella María De Jesús Napán CarbajalNo ratings yet
- Parkinsonismo VascularDocument9 pagesParkinsonismo VascularAna María Saldaña BenavidesNo ratings yet
- Movement Disorder in ChildrenDocument35 pagesMovement Disorder in Childrenstandar 1 neuroNo ratings yet
- Frontal LobeDocument63 pagesFrontal LobeDevdeep Roy ChowdhuryNo ratings yet
- Phillips 2008Document25 pagesPhillips 2008Donald Cabrera AstudilloNo ratings yet
- ParkinsonsDocument171 pagesParkinsonsSamyukta BudumuruNo ratings yet
- Neuro Basal GangliaDocument14 pagesNeuro Basal GangliaFu Xiao ShanNo ratings yet
- Pocket Neurology (Pocket Notebook Series) (PDFDrive)Document659 pagesPocket Neurology (Pocket Notebook Series) (PDFDrive)Kirstine Gail Zingalawa-EfacNo ratings yet
- Https Emedicine - Medscape.com Article 1831191-PrintDocument59 pagesHttps Emedicine - Medscape.com Article 1831191-PrintNoviatiPrayangsariNo ratings yet
- ADHD - Barkley PDFDocument6 pagesADHD - Barkley PDFKarla MollinedoNo ratings yet
- MDthesis PDFDocument174 pagesMDthesis PDFFifi RohmatinNo ratings yet
- Control of Movement by The Brain: Fakultas Kedokteran USUDocument12 pagesControl of Movement by The Brain: Fakultas Kedokteran USUWinda Adelia LubisNo ratings yet
- Case Study on Dementia: Physical Examination FindingsDocument47 pagesCase Study on Dementia: Physical Examination FindingsIrish Jane Bayle CubilloNo ratings yet
- Biological Psychology 12Th Edition Kalat Test Bank Full Chapter PDFDocument55 pagesBiological Psychology 12Th Edition Kalat Test Bank Full Chapter PDFElizabethRuizrxka100% (12)
- Neurological ExaminationDocument216 pagesNeurological Examinationkid_latigo100% (4)
- Arthur MacNeill Horton Jr. EdD ABPP ABPN, Lawrence C. Hartlage PHD ABPP ABPN - Handbook of Forensic Neuropsychology-Springer Publishing Company (2003) PDFDocument569 pagesArthur MacNeill Horton Jr. EdD ABPP ABPN, Lawrence C. Hartlage PHD ABPP ABPN - Handbook of Forensic Neuropsychology-Springer Publishing Company (2003) PDF'Minerva AlejandraNo ratings yet
- Integrative Neuroscience BringingDocument269 pagesIntegrative Neuroscience BringinghalleyworldNo ratings yet
- 2018 Article 1130Document30 pages2018 Article 1130imkaikin001No ratings yet
- The Limbic SystemDocument7 pagesThe Limbic Systemkerima juliaNo ratings yet
- Neurohormonal Regulation of Body FunctionsDocument34 pagesNeurohormonal Regulation of Body FunctionsjimmyNo ratings yet
- The Nigrostriatal PathwayDocument13 pagesThe Nigrostriatal Pathwayapi-534201968No ratings yet
- Basal GangliaDocument50 pagesBasal Ganglialion2chNo ratings yet
- American Association For The Advancement of ScienceDocument7 pagesAmerican Association For The Advancement of SciencecaeliumNo ratings yet