You might also like
- Berkshire HRTDocument7 pagesBerkshire HRTpiNo ratings yet
- Chapter 26Document84 pagesChapter 26Johanna Erazo Padilla100% (1)
- Hydatidiform MoleDocument10 pagesHydatidiform MoleLisa TurnerNo ratings yet
- Gestational Trophoblastic DiseasesDocument43 pagesGestational Trophoblastic DiseasesAnironOrion100% (1)
- GTD Case StudyDocument9 pagesGTD Case StudyZnarf Izlah Sadanreb100% (1)
- Vesicular MoleDocument46 pagesVesicular Moledhisazainita0% (1)
- Gestational Trophoblastic Disease (GTD) : Ahmed Refaat Abd ElzaherDocument41 pagesGestational Trophoblastic Disease (GTD) : Ahmed Refaat Abd ElzaherJessica NadiaNo ratings yet
- Hydatifor M Mole: By: Namita Arya Asst. Lecturer PDMSNCDocument27 pagesHydatifor M Mole: By: Namita Arya Asst. Lecturer PDMSNCnamitaNo ratings yet
- Ectopic PregnancyDocument3 pagesEctopic PregnancyMary Anne Yap100% (1)
- Hydatidiform Mole Study GuideDocument4 pagesHydatidiform Mole Study GuideCarl Elexer Cuyugan AnoNo ratings yet
- Pregnancy and TBDocument24 pagesPregnancy and TBRoza MaulindraNo ratings yet
- Hyperemesis GravidarumDocument16 pagesHyperemesis GravidarumGracy Casaña100% (2)
- Ectopic Pregnancy - OMDocument9 pagesEctopic Pregnancy - OMrheindNo ratings yet
- PID: Understanding Pelvic Inflammatory DiseaseDocument34 pagesPID: Understanding Pelvic Inflammatory Diseaseraed faisalNo ratings yet
- 3 (OB Cases)Document267 pages3 (OB Cases)Sharyl Plan SarominesNo ratings yet
- Abnormal PuerperiumDocument21 pagesAbnormal PuerperiumNatukunda DianahNo ratings yet
- E Maternal Adaptations To PregnancyDocument27 pagesE Maternal Adaptations To PregnancyGeraldine PatayanNo ratings yet
- OBG DrugsDocument30 pagesOBG DrugsSANANo ratings yet
- High Risk PregnancyDocument14 pagesHigh Risk PregnancyJezrael PueblosNo ratings yet
- Ectopic PregnancyDocument3 pagesEctopic PregnancyforbiddenleiNo ratings yet
- Multiple PregnancyDocument20 pagesMultiple PregnancySelma FraNo ratings yet
- Case StudyDocument48 pagesCase Studysimbarashe tangwadzanaNo ratings yet
- Normal PuerperiumDocument23 pagesNormal Puerperiumnaga maniNo ratings yet
- Clinical Teaching 4PEUPERAL SEPSISDocument5 pagesClinical Teaching 4PEUPERAL SEPSISAjit M Prasad PrasadNo ratings yet
- Abortion Definition, Types, Causes and ManagementDocument77 pagesAbortion Definition, Types, Causes and ManagementPadmaNo ratings yet
- Gestational Diabetus MellitusDocument28 pagesGestational Diabetus MellitusSanthosh.S.U100% (1)
- Gynaecological Procedure SeminarDocument33 pagesGynaecological Procedure SeminarTausif HaqueNo ratings yet
- Dermoid CystDocument8 pagesDermoid CystMohamed Hazem ElfollNo ratings yet
- Pathophysiology of Molar PregnancyDocument1 pagePathophysiology of Molar PregnancyFilipinas BelzaNo ratings yet
- AbortionDocument62 pagesAbortionRaj KumarNo ratings yet
- Gestational Trophoblastic DiseaseDocument5 pagesGestational Trophoblastic DiseaseWarshak NathNo ratings yet
- Partograph Monitoring Labor ProgressDocument65 pagesPartograph Monitoring Labor ProgressAmyAgustinNo ratings yet
- Importance of structured teaching on gestational hypertensionDocument18 pagesImportance of structured teaching on gestational hypertensionمالك مناصرةNo ratings yet
- Hiv and Aids in ChildrenDocument36 pagesHiv and Aids in ChildrenKazau FwalangaNo ratings yet
- Complications of Third Stage of LabourDocument7 pagesComplications of Third Stage of LabourDeepaRamani100% (1)
- Hydatidiform Mole/ Molar Pregnancy: College of Health SciencesDocument11 pagesHydatidiform Mole/ Molar Pregnancy: College of Health SciencesAngelu Gabrielle CastroNo ratings yet
- Maternal Adaptation To PregnancyDocument57 pagesMaternal Adaptation To PregnancyQuolette Constante100% (6)
- Psychological Changes of PregnancyDocument6 pagesPsychological Changes of PregnancyMarie PotayreNo ratings yet
- H MoleDocument35 pagesH MoleAris Resurreccion100% (1)
- Abnormal Uterine ActionDocument33 pagesAbnormal Uterine ActionRadwa Ebed100% (1)
- Intrauterine Fetal DemiseDocument7 pagesIntrauterine Fetal DemiseElaisa Mae Delos SantosNo ratings yet
- Understanding HIV and HAART ManagementDocument33 pagesUnderstanding HIV and HAART ManagementWill CheahNo ratings yet
- Material On PHYSIOLOGICAL CHANGES DURING PREGNANCYDocument21 pagesMaterial On PHYSIOLOGICAL CHANGES DURING PREGNANCYAnuradha MauryaNo ratings yet
- Ectopic PregnancyDocument4 pagesEctopic PregnancyJovie Anne BorjaNo ratings yet
- The Incompetent Cervix 2Document30 pagesThe Incompetent Cervix 2api-3705046100% (3)
- Postpartum ComplicationsDocument21 pagesPostpartum ComplicationsRoccabeth Villanueva100% (1)
- Definition, Types, and Management of Placenta AccretaDocument3 pagesDefinition, Types, and Management of Placenta AccretaFigueroa John ReyNo ratings yet
- Threatened AbortionDocument1 pageThreatened AbortionKEn PilapilNo ratings yet
- Managing Pelvic Inflammatory DiseaseDocument9 pagesManaging Pelvic Inflammatory DiseaseanweshaNo ratings yet
- POLYHYDRAMNIOSDocument2 pagesPOLYHYDRAMNIOSyxly imperialNo ratings yet
- Breast AbscessDocument2 pagesBreast AbscessJoanna Agustin0% (1)
- Pre-Eclampsia, Eclampsia and HELLP SyndromeDocument15 pagesPre-Eclampsia, Eclampsia and HELLP SyndromehendraNo ratings yet
- RZ - SGH Ok Polyhydramnios and OligohydramniosDocument24 pagesRZ - SGH Ok Polyhydramnios and OligohydramniosBilly DarismaNo ratings yet
- Abnormalities of The Puerperium: Puerperal PyrexiaDocument28 pagesAbnormalities of The Puerperium: Puerperal Pyrexiadrravindermehetrey100% (2)
- Hepatitis B in Pregnancy: Global Importance and Need for ControlDocument42 pagesHepatitis B in Pregnancy: Global Importance and Need for ControlAbraham ChiuNo ratings yet
- Purperal InfectionsDocument69 pagesPurperal InfectionsBeulah DasariNo ratings yet
- Preconception Care Presentation SlidesDocument15 pagesPreconception Care Presentation SlidesLucy AsconaNo ratings yet
- Complications of Pregnancy - EM - 2019voiceDocument60 pagesComplications of Pregnancy - EM - 2019voicekeoshaNo ratings yet
- The High Risk PregnancyDocument23 pagesThe High Risk Pregnancynursereview100% (3)
- Cervicitis Causes, Symptoms, Diagnosis and TreatmentDocument7 pagesCervicitis Causes, Symptoms, Diagnosis and TreatmentElaisa Mae Delos SantosNo ratings yet
- Spontaneous MiscarriageDocument14 pagesSpontaneous MiscarriageGomez VanessaNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Dr. Ni Made Indri - CC For Ovulation InductionDocument26 pagesDr. Ni Made Indri - CC For Ovulation InductionAPOTEK Sarah FarmaNo ratings yet
- Prenatal Management (Part 4)Document17 pagesPrenatal Management (Part 4)Austine James Sabenicio PantiloNo ratings yet
- HORMON REPRODUKSI DAN SIKLUS HAID Prof. Dr. Dr. Nusratuddin Abdullah, SP - OG (K) MARSDocument21 pagesHORMON REPRODUKSI DAN SIKLUS HAID Prof. Dr. Dr. Nusratuddin Abdullah, SP - OG (K) MARStenri olaNo ratings yet
- Bapt ToolDocument11 pagesBapt ToolShafiNo ratings yet
- Bipolar DisorderDocument4 pagesBipolar DisorderDeepak BamNo ratings yet
- Ncma217 Performancetask#5 TinioDocument7 pagesNcma217 Performancetask#5 TinioAndhee Mae TinioNo ratings yet
- PuerperiumDocument12 pagesPuerperiumsubhro kanti duttaNo ratings yet
- PMTCTDocument52 pagesPMTCTAbdissaTadeseNo ratings yet
- Breast CareDocument20 pagesBreast CareAna100% (3)
- Rotation Plan Obg BSC 4 LatestDocument7 pagesRotation Plan Obg BSC 4 Latestkamaljit kaurNo ratings yet
- Assignment On Family PlanningDocument8 pagesAssignment On Family Planningpiyush075171% (7)
- Iloilo City Regulation Ordinance 2015-163Document5 pagesIloilo City Regulation Ordinance 2015-163Iloilo City CouncilNo ratings yet
- Kode Pintar Icd 10Document60 pagesKode Pintar Icd 10Nur LailaNo ratings yet
- Human Reproduction SystemsDocument29 pagesHuman Reproduction SystemsSaku786No ratings yet
- Presentation-WPS OfficeDocument47 pagesPresentation-WPS OfficeJeffrey JasarenoNo ratings yet
- Advanced Maternal Age & PregnancyDocument67 pagesAdvanced Maternal Age & PregnancyMa Pilar Peñaflor AñonuevoNo ratings yet
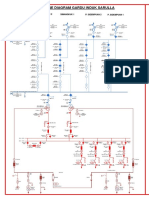
- SLD Gi SarullaDocument1 pageSLD Gi SarullasacilatwaeNo ratings yet
- Gyn Infertility PresentationDocument30 pagesGyn Infertility Presentationapi-507364479No ratings yet
- Effect of Whatsapp Reminder On Antenatal Care RevisitDocument11 pagesEffect of Whatsapp Reminder On Antenatal Care RevisitElita NapiaNo ratings yet
- ContraceptionDocument23 pagesContraceptionJhApz Vrzs ÆmnNo ratings yet
- KodefDocument45 pagesKodefWann FarhannaNo ratings yet
- EINCDocument1 pageEINCRaidis PangilinanNo ratings yet
- Case Study For Uterine-CancerDocument9 pagesCase Study For Uterine-CancerGabbii CincoNo ratings yet
- Obstetrics and Gynecology ClinicsDocument201 pagesObstetrics and Gynecology ClinicsaedicofidiaNo ratings yet
- Smith Dysmenorrhea and Menorrhagia - A Clinician's Guide PDFDocument163 pagesSmith Dysmenorrhea and Menorrhagia - A Clinician's Guide PDFsafiraNo ratings yet
- Perdarahan Uterus AbnormalDocument15 pagesPerdarahan Uterus Abnormalarfiah100% (1)
- Pengaruh Pijat Oksitosin Terhadap Kelancaran ASIDocument10 pagesPengaruh Pijat Oksitosin Terhadap Kelancaran ASIFira SyahputriNo ratings yet
- Obstetrics N Gynaec Nursing PDFDocument12 pagesObstetrics N Gynaec Nursing PDFSijo Muthukad M100% (1)