You might also like
- IV Injections and InfusionsDocument2 pagesIV Injections and InfusionsFrancis Lawrence AlexanderNo ratings yet
- NABH Staff RatioDocument1 pageNABH Staff RatioRetteri KUMARANNo ratings yet
- Seminar Topic - Job Description of Departmental SisterDocument18 pagesSeminar Topic - Job Description of Departmental Sistershubham rathod0% (1)
- Nursing AuditDocument26 pagesNursing AuditJoe ShewaleNo ratings yet
- Verbal Order PolicyDocument4 pagesVerbal Order PolicyAruna HarikrishnanNo ratings yet
- Back CareDocument56 pagesBack CareSandeep Maan100% (2)
- Synopsis - Nursing ExcellenceDocument19 pagesSynopsis - Nursing ExcellenceD. Gandhiraj100% (1)
- Clinical TeachingDocument29 pagesClinical TeachingJeonoh Florida100% (2)
- School of Nursing Sciences and Research Sharda University: Problem StatementDocument2 pagesSchool of Nursing Sciences and Research Sharda University: Problem StatementBhawna JoshiNo ratings yet
- Hospital OrientationDocument82 pagesHospital OrientationDondee Pamposa100% (2)
- Evidence Based Practice in ObstetricsDocument17 pagesEvidence Based Practice in ObstetricsAnn Merlin JobinNo ratings yet
- Nursing ProcessDocument45 pagesNursing ProcessSukmaErfiana100% (1)
- Final Problem Statement EctDocument2 pagesFinal Problem Statement EctRahul DamorNo ratings yet
- Professor CollegeDocument3 pagesProfessor CollegeAnusha VergheseNo ratings yet
- DialysisDocument20 pagesDialysisSiwani rai100% (1)
- FAMILY PLanning FinalDocument23 pagesFAMILY PLanning FinalLebo Ramokolo100% (1)
- Effectiveness of Planned Teaching Programme On Knowledge of Emergency Drugs Among Staff NursesDocument4 pagesEffectiveness of Planned Teaching Programme On Knowledge of Emergency Drugs Among Staff NursesRumela Ganguly ChakrabortyNo ratings yet
- Nursing EmpowermentDocument1 pageNursing Empowermentsudhakar pNo ratings yet
- Registration FormDocument5 pagesRegistration FormSreejith Kelakam100% (1)
- Preop ChecklistDocument2 pagesPreop ChecklistJan Federick BantayNo ratings yet
- NURSING ROUNDsDocument8 pagesNURSING ROUNDsHeryani AnikNo ratings yet
- STD Control ProgrammeDocument1 pageSTD Control Programmeangayarkanni100% (1)
- Title Page: Title of The Article: "A Study To Assess The Effectiveness of Structured Teaching Programme OnDocument9 pagesTitle Page: Title of The Article: "A Study To Assess The Effectiveness of Structured Teaching Programme OnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Amogha Institute of Professional and Techincal Education: B.SC Nursing 4 Year Midwifery and Obstetrical NursingDocument2 pagesAmogha Institute of Professional and Techincal Education: B.SC Nursing 4 Year Midwifery and Obstetrical Nursingannu panchalNo ratings yet
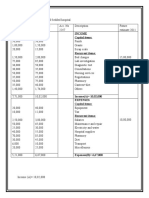
- Income Capital ItemsDocument2 pagesIncome Capital ItemsDeepti KukretiNo ratings yet
- NCM 107Document7 pagesNCM 107Jose Jumamoy100% (1)
- Lecture-18 Obstructed LaborDocument8 pagesLecture-18 Obstructed LaborMadhu Sudhan PandeyaNo ratings yet
- Joint Director of NursingDocument2 pagesJoint Director of NursingAnusha VergheseNo ratings yet
- Handing and Taking OverDocument8 pagesHanding and Taking OverDivya ThomasNo ratings yet
- 05 Developing Standards ofDocument8 pages05 Developing Standards ofSachin SinghNo ratings yet
- Autonomy and AccountabilityDocument3 pagesAutonomy and Accountabilityakashdeep rathodNo ratings yet
- First Referral UnitDocument24 pagesFirst Referral Unitjay5ar5jamorabon5torNo ratings yet
- By:-Firoz Qureshi Dept. Psychiatric NursingDocument46 pagesBy:-Firoz Qureshi Dept. Psychiatric NursingrajeshwariNo ratings yet
- Primary Nursing Care .Document6 pagesPrimary Nursing Care .Patel Amee100% (1)
- CURRICULUM RESEARCH IN NURSING - WordDocument4 pagesCURRICULUM RESEARCH IN NURSING - WordSMITHA JOSENo ratings yet
- Practical 3 PDFDocument6 pagesPractical 3 PDFPriyanjali Saini100% (1)
- Clinical Learning ContractDocument3 pagesClinical Learning ContractKaragire vedasteNo ratings yet
- OREM'SDocument32 pagesOREM'SJoji JohnNo ratings yet
- Augmentation of Labour: Nabhan A, Boulvain MDocument8 pagesAugmentation of Labour: Nabhan A, Boulvain MMade SuryaNo ratings yet
- Taking A 12 Lead ECGDocument4 pagesTaking A 12 Lead ECGmadiehahNo ratings yet
- A Study To Evaluate The Effectiveness of Structured Teaching Program On Knowledge and Practice Regarding Kangaroo Mother Care Among Post Natal Mothers Having Low Birth Weight Babies 1Document9 pagesA Study To Evaluate The Effectiveness of Structured Teaching Program On Knowledge and Practice Regarding Kangaroo Mother Care Among Post Natal Mothers Having Low Birth Weight Babies 1Manisa ParidaNo ratings yet
- About Clinical Instructors Evaluating Nursing StudentsDocument22 pagesAbout Clinical Instructors Evaluating Nursing Studentsrex_tubana50% (2)
- 3 - Diagnosis of PregnancyDocument5 pages3 - Diagnosis of PregnancyM7 AlfatihNo ratings yet
- C12 P13 TubectomyDocument24 pagesC12 P13 TubectomyRaviKurleNo ratings yet
- Pediatric Nursing and Nursing theory-YADocument31 pagesPediatric Nursing and Nursing theory-YALuthi PratiwiNo ratings yet
- Eye Irrigation ChecklistDocument3 pagesEye Irrigation ChecklistAlma Janella TOSINONo ratings yet
- Evaluationppt 110926211536 Phpapp01Document35 pagesEvaluationppt 110926211536 Phpapp01Seema VashishtNo ratings yet
- Admission & Discharge FONDocument43 pagesAdmission & Discharge FONDr.Nisha Prasad.No ratings yet
- Knowledge and Practice Towards Care and MaintenancDocument7 pagesKnowledge and Practice Towards Care and MaintenancyunishaNo ratings yet
- MSC Question PaperDocument6 pagesMSC Question PaperAnusha VergheseNo ratings yet
- Administrative Applications in Nursing 09Document23 pagesAdministrative Applications in Nursing 09ramroum18No ratings yet
- Bleeding Disorders FinalDocument35 pagesBleeding Disorders FinalsanthiyasandyNo ratings yet
- Con Mission, Vision, ObjectivesDocument1 pageCon Mission, Vision, ObjectivesMelchor Felipe SalvosaNo ratings yet
- Intensive Care Nursing Lecture NotesDocument5 pagesIntensive Care Nursing Lecture NotesMark Russel Sean LealNo ratings yet
- Patient Assignment MethodDocument48 pagesPatient Assignment Methodsathya Arunkumar100% (1)
- IPSGDocument29 pagesIPSGShermaida Basirul100% (1)
- Knowledge Regarding Skin Banking Among Student NursesDocument5 pagesKnowledge Regarding Skin Banking Among Student NursesAnonymous izrFWiQNo ratings yet
- Breast Care ChecklistDocument3 pagesBreast Care ChecklistNeil Nette ReynaldoNo ratings yet
- HMISDocument34 pagesHMISavinash dhameriyaNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Closing Remarks - Nursing Midwifery LeadershipDocument19 pagesClosing Remarks - Nursing Midwifery LeadershipJhpiegoNo ratings yet
- GE Foundation Awards Jhpiego $2.3 Million To Accelerate Global Health InnovationsDocument2 pagesGE Foundation Awards Jhpiego $2.3 Million To Accelerate Global Health InnovationsJhpiegoNo ratings yet
- Seizing The Opportunity - Working With Adolescent Boys For An HIV-free Generation"Document14 pagesSeizing The Opportunity - Working With Adolescent Boys For An HIV-free Generation"JhpiegoNo ratings yet
- Cervical Cancer Screening - JhpiegoDocument15 pagesCervical Cancer Screening - JhpiegoJhpiego100% (1)
- Spatial Mapping Results in a Successful Large-Scale Voluntary Medical Male Circumcision (VMMC) Campaign: Using GIS Data for Decision-Making Positively Impacts the VMMC Scale-Up in Iringa and Njombe Regions of TanzaniaDocument1 pageSpatial Mapping Results in a Successful Large-Scale Voluntary Medical Male Circumcision (VMMC) Campaign: Using GIS Data for Decision-Making Positively Impacts the VMMC Scale-Up in Iringa and Njombe Regions of TanzaniaJhpiegoNo ratings yet
- Community Health Workers Creating Family Planning Social Networks Through Satisified ClientsDocument15 pagesCommunity Health Workers Creating Family Planning Social Networks Through Satisified ClientsJhpiegoNo ratings yet
- Capturing A Missed Opportunity Through Postpartum Intrauterine Contraceptive Device (PPIUCD) in Ethiopia: Experience of The Maternal and Child Health Integrated Program (MCHIP)Document13 pagesCapturing A Missed Opportunity Through Postpartum Intrauterine Contraceptive Device (PPIUCD) in Ethiopia: Experience of The Maternal and Child Health Integrated Program (MCHIP)JhpiegoNo ratings yet
- Date/Time: Thursday, November 14, 2013 Session: 2.2.11 Family Planning and Quality of CareDocument2 pagesDate/Time: Thursday, November 14, 2013 Session: 2.2.11 Family Planning and Quality of CareJhpiegoNo ratings yet
- Screening For Maternal Anemia: A Low-Cost Solution For A Persistent Global Health ChallengeDocument1 pageScreening For Maternal Anemia: A Low-Cost Solution For A Persistent Global Health ChallengeJhpiegoNo ratings yet
- Improving Maternal Child Health (MCH) ServicesDocument22 pagesImproving Maternal Child Health (MCH) ServicesJhpiegoNo ratings yet
- Course Pack - Cost Accounting Bba 2 (1) - Revised - 5th Jan 2024Document124 pagesCourse Pack - Cost Accounting Bba 2 (1) - Revised - 5th Jan 2024Sapna Prashant SharmaNo ratings yet
- BBC News - AFRICA - Africa's 'Greatest Explorer'Document4 pagesBBC News - AFRICA - Africa's 'Greatest Explorer'Nuqman Tehuti El100% (1)
- Cantilever Lab IB Physics IADocument6 pagesCantilever Lab IB Physics IAChelci Erin Houston100% (2)
- Character Strengths Bunting ResourceDocument34 pagesCharacter Strengths Bunting ResourcewarrenNo ratings yet
- Philippine Statistics Authority: 2020 Census of Population and Housing (CPH) Narrative Report Municipality ofDocument4 pagesPhilippine Statistics Authority: 2020 Census of Population and Housing (CPH) Narrative Report Municipality ofGina silvaNo ratings yet
- SwitraDocument6 pagesSwitradrbhaveshpNo ratings yet
- Problem Set 8Document3 pagesProblem Set 8JonahJunior0% (1)
- Seven Essential COmponents To A Marketting PlanDocument1 pageSeven Essential COmponents To A Marketting PlanGeneTearBodgesNo ratings yet
- Customer Service Department and Clients Satisfaction: An Empirical Study of Commercial Bank of Surkhet, ValleyDocument7 pagesCustomer Service Department and Clients Satisfaction: An Empirical Study of Commercial Bank of Surkhet, ValleyThe IjbmtNo ratings yet
- Projecct LETRADocument8 pagesProjecct LETRAKenneth Roy Matuguina50% (2)
- Teacher Education: Quirino State UniversityDocument11 pagesTeacher Education: Quirino State UniversityNoralyn Ulnagan ParditoNo ratings yet
- Gtaw NC Ii DocsDocument100 pagesGtaw NC Ii DocsAris BulaongNo ratings yet
- The Influence of Corporate Social Responsibility On Incumbent Employees: A Meta-Analytic Investigation of The Mediating and Moderating MechanismsDocument33 pagesThe Influence of Corporate Social Responsibility On Incumbent Employees: A Meta-Analytic Investigation of The Mediating and Moderating MechanismsDuaa ZahraNo ratings yet
- The Six Types of Socratic QuestionsDocument2 pagesThe Six Types of Socratic QuestionsBuketNo ratings yet
- Changing The Cotton Landscape in Pakistan - Forrester - 2009Document49 pagesChanging The Cotton Landscape in Pakistan - Forrester - 2009Ahsan 11100% (1)
- Borrero 2008, Extincion MegafaunaDocument6 pagesBorrero 2008, Extincion MegafaunaHernanNo ratings yet
- Stages of EIADocument31 pagesStages of EIAAstra CardinalNo ratings yet
- Eruption! Discussion GuideDocument5 pagesEruption! Discussion GuideHoughton Mifflin HarcourtNo ratings yet
- Curr - DevDocument13 pagesCurr - DevPaulAliboghaNo ratings yet
- Answer: Put It Diagonally in A Cubical Box 1 Yard On A SideDocument6 pagesAnswer: Put It Diagonally in A Cubical Box 1 Yard On A Sideiamcerbzjr100% (1)
- Case Report TemplateDocument3 pagesCase Report TemplateAgatha Pralita KusumawardhiniNo ratings yet
- Module in Elementary Statistics and Probability With LaboratoryDocument15 pagesModule in Elementary Statistics and Probability With LaboratoryMonec JalandoniNo ratings yet
- Human Resource Management Practices in India ProjectDocument7 pagesHuman Resource Management Practices in India ProjectRam KishorNo ratings yet
- Design of ExperimentDocument49 pagesDesign of ExperimentMuhammad Insan KamilNo ratings yet
- Reflection Exam Final 1Document5 pagesReflection Exam Final 1api-584147825No ratings yet
- PLC Mathematics Year 2Document5 pagesPLC Mathematics Year 2AndyKongNo ratings yet
- Generic Skill AssesmentDocument110 pagesGeneric Skill Assesmentkang-aipNo ratings yet
- Multicultural Dance WebquestDocument3 pagesMulticultural Dance Webquestapi-398534676No ratings yet
- 1333482681.637اختبار تورانس المختصر للتفكير الابداعيDocument39 pages1333482681.637اختبار تورانس المختصر للتفكير الابداعيsokysewNo ratings yet
- Online Shopping Drivers and Barriers For Older Adults-Age and GenderDocument11 pagesOnline Shopping Drivers and Barriers For Older Adults-Age and GenderAntania HarunNo ratings yet