You might also like
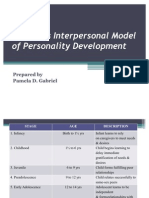
- Sullivan's Interpersonal Model of Personality DevelopmentDocument8 pagesSullivan's Interpersonal Model of Personality DevelopmentPamDavidGabrielNo ratings yet
- Mentally Challenged ChildrenDocument4 pagesMentally Challenged ChildrenSanthosh.S.UNo ratings yet
- Crisis Intervention (Mrs. Jeena Jose) NS: IntrodutionDocument4 pagesCrisis Intervention (Mrs. Jeena Jose) NS: IntrodutionManisha ThakurNo ratings yet
- Problem of Empty Nest Syndrome: An Analysis and Suggestions To Bridle ItDocument4 pagesProblem of Empty Nest Syndrome: An Analysis and Suggestions To Bridle ItBoz Ralph PentinioNo ratings yet
- Stages of Human Development by Erik Erikson and Four Personality Types Merill-Reid ModelDocument11 pagesStages of Human Development by Erik Erikson and Four Personality Types Merill-Reid ModelFrich Delos Santos PeñaNo ratings yet
- Factors Affecting Mental HealthDocument4 pagesFactors Affecting Mental HealthGeorge BendanilloNo ratings yet
- Unit 6 B Therapeutic Relationship-1Document36 pagesUnit 6 B Therapeutic Relationship-1Nayel ZeeshanNo ratings yet
- Mini Mental Status ExamDocument10 pagesMini Mental Status ExamFrench Pastolero-ManaloNo ratings yet
- Communicating With Patients From Different Cultural BackgroundDocument24 pagesCommunicating With Patients From Different Cultural BackgroundRiska Aprilia100% (1)
- Characteristics of CounsellingDocument9 pagesCharacteristics of Counsellingrashi sharmaNo ratings yet
- Hildgard PeplauDocument31 pagesHildgard PeplauHazel LezahNo ratings yet
- Maternal Deprivation Lesson PlanDocument18 pagesMaternal Deprivation Lesson PlanSAYMABANUNo ratings yet
- Coping With Loss Griving 0 DeathDocument16 pagesCoping With Loss Griving 0 DeathSandhya Gupta100% (1)
- Psychological Changes, Danger Signs, DiscomfortsDocument21 pagesPsychological Changes, Danger Signs, DiscomfortsPasay Trisha Faye Y.No ratings yet
- Communication, Ipr, Group Dynamics and Organisational BehaviourDocument30 pagesCommunication, Ipr, Group Dynamics and Organisational BehaviourSrd RchNo ratings yet
- Therapeutic CommunicationDocument20 pagesTherapeutic CommunicationMakanjuola Osuolale John0% (1)
- Case PresentationDocument6 pagesCase Presentationاكرم صالحين100% (1)
- Group DynamicsDocument5 pagesGroup Dynamicsnehatiwari1805100% (1)
- The Psychiatric Mental Status Exam (MSE)Document4 pagesThe Psychiatric Mental Status Exam (MSE)dev100% (1)
- Anorexia Vs BulimiaDocument19 pagesAnorexia Vs BulimiaNylia AtibiNo ratings yet
- Prepared By:-Ghada Almukhaini Supervised By: - PROF - DR. ELHAM FAYADHDocument61 pagesPrepared By:-Ghada Almukhaini Supervised By: - PROF - DR. ELHAM FAYADHGhada Almukhaini100% (1)
- Pamela G ReedDocument3 pagesPamela G ReedGabNo ratings yet
- Assessing Mental StatusDocument13 pagesAssessing Mental StatusKadiza ArabiNo ratings yet
- Interpersonal PsychotherapyDocument21 pagesInterpersonal PsychotherapyDr. Jayesh PatidarNo ratings yet
- Adolescent DevelopmentDocument29 pagesAdolescent DevelopmentNiwematsiko ProfitNo ratings yet
- Peer Group Presentation On: Recreational Therapy Play Therapy Music TherapyDocument10 pagesPeer Group Presentation On: Recreational Therapy Play Therapy Music TherapyMonikaNo ratings yet
- Developmental MilestonesDocument2 pagesDevelopmental Milestonesdanee し100% (1)
- Family Development Cycle: Mrs - Neethu Vincent Asst Professor KVM College of NursingDocument22 pagesFamily Development Cycle: Mrs - Neethu Vincent Asst Professor KVM College of NursingNeethu VincentNo ratings yet
- Care of Mentally ChallengedDocument71 pagesCare of Mentally ChallengedTilarupa Bhattarai100% (1)
- MilieuDocument17 pagesMilieuAntro BerrinNo ratings yet
- Sathish Rajamani Milieu TherapyDocument4 pagesSathish Rajamani Milieu TherapySathish Rajamani0% (1)
- Mental Health Team & New Trends in PNDocument23 pagesMental Health Team & New Trends in PN27. Ramila ManvarNo ratings yet
- The Family As A UnitDocument6 pagesThe Family As A UnitSharmaine Grace FlorigNo ratings yet
- Psy - Nursing Care Plan - Therapeutic CommunicationDocument6 pagesPsy - Nursing Care Plan - Therapeutic CommunicationCarmen Angela DusaranNo ratings yet
- Conduct Disorder PPT - K. Elise ParkerDocument17 pagesConduct Disorder PPT - K. Elise Parkerepaka02No ratings yet
- Holistic Nursing CareDocument14 pagesHolistic Nursing CaremujionoNo ratings yet
- General Survey, Mental Status Exam, andDocument25 pagesGeneral Survey, Mental Status Exam, andjazzreign50% (2)
- Post Partum PsychosisDocument29 pagesPost Partum Psychosispreeti sharmaNo ratings yet
- Family TherapyDocument15 pagesFamily TherapyAshish_Singh_5126100% (1)
- Oppositional Defiant Disorder OddDocument10 pagesOppositional Defiant Disorder Oddapi-360330020No ratings yet
- Interpersonal RelationshipDocument22 pagesInterpersonal RelationshipnoryhoneyNo ratings yet
- Techniques of CounsellingDocument3 pagesTechniques of CounsellingVictini codeNo ratings yet
- Group TherapyDocument4 pagesGroup TherapyMuhammad ThohariNo ratings yet
- Topographic TheoryDocument7 pagesTopographic TheoryAdrishya0% (1)
- Behavior Therapy: Presented By: Saba AhmedDocument38 pagesBehavior Therapy: Presented By: Saba AhmedRana Ahmad GulraizNo ratings yet
- A Personal Reflection On My Experience As A Mental Health Nurse in New ZealandDocument5 pagesA Personal Reflection On My Experience As A Mental Health Nurse in New ZealandMezil NazarenoNo ratings yet
- Breech Presentation-Muhammad NzarDocument26 pagesBreech Presentation-Muhammad NzarRaman Khdr QaladzayNo ratings yet
- Psychoanalytic TherapyDocument7 pagesPsychoanalytic Therapygellets balmoresNo ratings yet
- Nursing Care Plan For A Patient With SchizophreniaDocument14 pagesNursing Care Plan For A Patient With SchizophreniaJerilee SoCute WattsNo ratings yet
- Care of Dying PatientDocument27 pagesCare of Dying PatientAbinaya Ranganathan100% (1)
- Issues of Mental Health NursingDocument16 pagesIssues of Mental Health NursingElita FadhliNo ratings yet
- Concept of Man, Health and IllnessDocument2 pagesConcept of Man, Health and IllnessMicah HuanNo ratings yet
- Orem's TheoryDocument40 pagesOrem's TheoryREVATHI H KNo ratings yet
- Human Growth and DevelopmentDocument14 pagesHuman Growth and DevelopmentAllan SantosNo ratings yet
- Rehabilitation of Mentally Ill PatientsDocument4 pagesRehabilitation of Mentally Ill PatientsSusmita HalderNo ratings yet
- Conduct DisorderDocument4 pagesConduct DisorderPrakriti KohliNo ratings yet
- Psycho EducationDocument14 pagesPsycho EducationMaha LakshmiNo ratings yet
- Generalized Anxiety DisorderDocument8 pagesGeneralized Anxiety DisorderTanvi SharmaNo ratings yet
- Play Therapy: DefinitionDocument11 pagesPlay Therapy: DefinitionSeema YadavNo ratings yet
- World Health Champion Game Questions Ampamp Answers BRMDocument18 pagesWorld Health Champion Game Questions Ampamp Answers BRMSalem alarjaniNo ratings yet
- Eye Movement Desensitization and Reprocessing EMDRDocument5 pagesEye Movement Desensitization and Reprocessing EMDRSalem alarjaniNo ratings yet
- Part A Mental Health and Psychosocial Support (MHPSS)Document5 pagesPart A Mental Health and Psychosocial Support (MHPSS)Salem alarjaniNo ratings yet
- Five Stages of Psychosexual DevelopmentDocument18 pagesFive Stages of Psychosexual DevelopmentSalem alarjaniNo ratings yet
- Salem E.S Al Arjani: Personal StatementDocument4 pagesSalem E.S Al Arjani: Personal StatementSalem alarjaniNo ratings yet
- Salem E.S Al Arjani: Personal StatementDocument3 pagesSalem E.S Al Arjani: Personal StatementSalem alarjaniNo ratings yet
- Alarjani CVDocument1 pageAlarjani CVSalem alarjaniNo ratings yet
- A.Arado - HBO Case Study - Humanized RobotsDocument3 pagesA.Arado - HBO Case Study - Humanized RobotsAdelson Arado83% (6)
- Taking Offense: Effects of Personality and Teasing History On Behavioral and Emotional Reactions To TeasingDocument49 pagesTaking Offense: Effects of Personality and Teasing History On Behavioral and Emotional Reactions To TeasingAlexandruTudorNo ratings yet
- Personal Development: Quarter 1-Module 5 Week 6&7Document16 pagesPersonal Development: Quarter 1-Module 5 Week 6&7Nikka Irah CamaristaNo ratings yet
- J Gray Viewpoint Matrix - Major Contributors in Gifted Education Sy21Document4 pagesJ Gray Viewpoint Matrix - Major Contributors in Gifted Education Sy21api-528983071No ratings yet
- Existential Psychology ReportDocument41 pagesExistential Psychology ReportJarem Phil Dolendo PalomataNo ratings yet
- Week 13 - Inter Cultural Competence & Inter Cultural AwarenessDocument25 pagesWeek 13 - Inter Cultural Competence & Inter Cultural AwarenessTuân NguyễnNo ratings yet
- Understandind The Links Between Social Media and DepressionDocument7 pagesUnderstandind The Links Between Social Media and DepressionSydney Frances AntiojoNo ratings yet
- Self Reflection Journal 1Document4 pagesSelf Reflection Journal 1api-436999044No ratings yet
- Communication For Children Should Be Age-Appropriate and Child-FriendlyDocument2 pagesCommunication For Children Should Be Age-Appropriate and Child-FriendlyChoirul AnwarNo ratings yet
- Case Study of Teenage PregnancyDocument16 pagesCase Study of Teenage PregnancyJanine LimjucoNo ratings yet
- 3 Cultural GenogramDocument11 pages3 Cultural GenogramJohn Stanley100% (2)
- Chapter 2 Peace EdDocument6 pagesChapter 2 Peace Edkea7078No ratings yet
- O'Shaughnessy, E. (2005) - Whose BionDocument4 pagesO'Shaughnessy, E. (2005) - Whose BionJulián Alberto Muñoz FigueroaNo ratings yet
- 2018 - Personality Disorders, Addictions and Psychopathy As Predictors of Criminal Behaviour in A Prison SampleDocument18 pages2018 - Personality Disorders, Addictions and Psychopathy As Predictors of Criminal Behaviour in A Prison SampleKarina FigueiredoNo ratings yet
- Curriculum Vitae - Fabian KiepeDocument2 pagesCurriculum Vitae - Fabian KiepeMichael SmithNo ratings yet
- Empployee Evaluation FormDocument2 pagesEmpployee Evaluation FormIrish AgpoonNo ratings yet
- Leson 7 (Sexuality in Marriage) PDFDocument6 pagesLeson 7 (Sexuality in Marriage) PDFhenryNo ratings yet
- San Francisco Parish School: Pauna ST., Del Remedio, Cardona, RizalDocument1 pageSan Francisco Parish School: Pauna ST., Del Remedio, Cardona, RizalTek CasoneteNo ratings yet
- Describe The Concept of Gender and Sex Recognize The Difference Between Gender and Sex Explain The Terms Gender DynamicsDocument4 pagesDescribe The Concept of Gender and Sex Recognize The Difference Between Gender and Sex Explain The Terms Gender DynamicsRexson Dela Cruz TagubaNo ratings yet
- Role of Effective Communication in Enhancing Employee Performance, Attitude and HappinessDocument18 pagesRole of Effective Communication in Enhancing Employee Performance, Attitude and HappinessPriyanshuNo ratings yet
- Core Behavioral Competencies Appendix d.3 Part IIDocument3 pagesCore Behavioral Competencies Appendix d.3 Part IIregine romero100% (2)
- LeadershipDocument44 pagesLeadershippanv_5254100% (1)
- K-12 Creativity-Innovation 2018Document55 pagesK-12 Creativity-Innovation 2018Allin John FranciscoNo ratings yet
- Biological Foundations of Human BehaviorDocument632 pagesBiological Foundations of Human BehaviorM sNo ratings yet
- Aiims - May - 17 - PsychiatryDocument3 pagesAiims - May - 17 - PsychiatryMinaz PatelNo ratings yet
- 18 Ubm 620-Consumer Behaviour Multiple Choice Questions: Unit-IDocument8 pages18 Ubm 620-Consumer Behaviour Multiple Choice Questions: Unit-IMadhu SharmaNo ratings yet
- Individual and SocietyDocument19 pagesIndividual and SocietyJoel EricNo ratings yet
- My Reflections On ShamanismDocument2 pagesMy Reflections On ShamanismPetru GusetNo ratings yet
- Chapter 4 - How A Society Is OrganizedDocument6 pagesChapter 4 - How A Society Is OrganizedJamesel VillaruzNo ratings yet
- Chapter Eight and Nine Life Skills and Interpersonal SkillsDocument122 pagesChapter Eight and Nine Life Skills and Interpersonal SkillsRuth K.No ratings yet