You might also like
- Scandinavian DefenceDocument4 pagesScandinavian DefenceGCY56No ratings yet
- French DefenceDocument1 pageFrench DefenceGCY56No ratings yet
- En Wikibooks Org Wiki Chess Opening Theory 1 E4 1 c5Document4 pagesEn Wikibooks Org Wiki Chess Opening Theory 1 E4 1 c5GCY56No ratings yet
- Sponsor St. Jude AMPLATZER ASO Panel Pack REDACTED PDFDocument35 pagesSponsor St. Jude AMPLATZER ASO Panel Pack REDACTED PDFGCY56No ratings yet
- Original London Tour MapDocument1 pageOriginal London Tour MapGCY56No ratings yet
- Sicilan VariationsDocument1 pageSicilan VariationsGCY56No ratings yet
- Radial Catheterization Postprocedural ComplicationsDocument2 pagesRadial Catheterization Postprocedural ComplicationsGCY56No ratings yet
- Sponsor St. Jude AMPLATZER ASO Panel Pack REDACTED PDFDocument35 pagesSponsor St. Jude AMPLATZER ASO Panel Pack REDACTED PDFGCY56No ratings yet
- Lien WaiverDocument1 pageLien WaiverGCY56No ratings yet
- Elec Safety WorkbookDocument16 pagesElec Safety WorkbookShahadat Hussain100% (1)
- 2011 May Trans Radial Arterial AccessDocument17 pages2011 May Trans Radial Arterial AccessGCY56No ratings yet
- Coronary Thrombus Classification and TreatmentDocument9 pagesCoronary Thrombus Classification and TreatmentGCY56No ratings yet
- Episodic To Chronic Migraine The Transformers: Disclosure: Reflects The Past 3 YearsDocument14 pagesEpisodic To Chronic Migraine The Transformers: Disclosure: Reflects The Past 3 YearsGCY56No ratings yet
- LinuxDocument2 pagesLinuxGCY56No ratings yet
- Tdi 3Document9 pagesTdi 3GCY56No ratings yet
- Vasc Chapter Le Venous AnatomyDocument11 pagesVasc Chapter Le Venous AnatomyGCY56No ratings yet
- HRJ - SkEye Introduction and TutorialDocument7 pagesHRJ - SkEye Introduction and TutorialGCY56No ratings yet
- Amtrak W21Document5 pagesAmtrak W21GCY56No ratings yet
- Meade DS2000Document44 pagesMeade DS2000GCY56No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Princeton 112 Manual PDFDocument4 pagesPrinceton 112 Manual PDFBenoitDeCoomanNo ratings yet
- SimBrief User Guide - Version 2.20.3Document54 pagesSimBrief User Guide - Version 2.20.3Natali MendozaNo ratings yet
- 0510 2013 Speaking (May June)Document20 pages0510 2013 Speaking (May June)Azliza YunusNo ratings yet
- Led Tube HF Ballast Compatibility List Q4 2021Document34 pagesLed Tube HF Ballast Compatibility List Q4 2021Iñaki Prego RamosNo ratings yet
- Experimental Investigation of The Stress-Stretch Behavior of EPDM Rubber With Loading Rate EffectsDocument20 pagesExperimental Investigation of The Stress-Stretch Behavior of EPDM Rubber With Loading Rate EffectsPaulo Venicio Alves VieiraNo ratings yet
- CIA Exam Preparation Part 1 Essentials of Internal AuditingDocument4 pagesCIA Exam Preparation Part 1 Essentials of Internal AuditingBin Saadun100% (1)
- Statement 1H0TFNJ Oct-2022Document3 pagesStatement 1H0TFNJ Oct-2022Mary MacLellanNo ratings yet
- Knowing My Values+Mindset - QuestionnaireDocument1 pageKnowing My Values+Mindset - QuestionnaireHungNo ratings yet
- March 21 InsertDocument8 pagesMarch 21 InsertBlack JackNo ratings yet
- Palestinian National IdentityDocument25 pagesPalestinian National IdentityFernando AdroverNo ratings yet
- NASA Fault Management HandbookDocument203 pagesNASA Fault Management HandbookManu MathewNo ratings yet
- A Most Odd Ratio - Interpreting and Describing Odds RatiosDocument5 pagesA Most Odd Ratio - Interpreting and Describing Odds RatiosAP KAPENo ratings yet
- Anthropology Pacific Island TrajectoriesDocument188 pagesAnthropology Pacific Island TrajectoriesBundit GrivijitrNo ratings yet
- Introduction to Transportation EngineeringDocument11 pagesIntroduction to Transportation EngineeringMuaz HararNo ratings yet
- END - Report GRP 4 PDFDocument169 pagesEND - Report GRP 4 PDFAmsathvany KanagasuntharasuwamyNo ratings yet
- BCN 4465 Outline-Fall 2016Document2 pagesBCN 4465 Outline-Fall 2016api-271970349No ratings yet
- Civil Rights Movement Journal Teachers VersionDocument2 pagesCivil Rights Movement Journal Teachers Versionapi-581217100No ratings yet
- 713g16 - Parts & Schematics ManualDocument58 pages713g16 - Parts & Schematics ManualВячеслав РубцовNo ratings yet
- Avm Imnr70 17aDocument2 pagesAvm Imnr70 17aRani HendrikusNo ratings yet
- Aslan 2017Document8 pagesAslan 2017Ana Maria Montoya GomezNo ratings yet
- Norwegian CH 1 - DuolingoDocument5 pagesNorwegian CH 1 - DuolingoDorin DamocNo ratings yet
- Stone ColumnDocument54 pagesStone ColumnFachreza AkbarNo ratings yet
- Sample SOD ConflictsDocument1 pageSample SOD ConflictsGulzar GhoshNo ratings yet
- Assessment Plan Computer Science and Information Systems Department Program/Course Assessment of The Five College-Wide Learning OutcomesDocument1 pageAssessment Plan Computer Science and Information Systems Department Program/Course Assessment of The Five College-Wide Learning Outcomesapi-24701542No ratings yet
- World History Final Study GuideDocument6 pagesWorld History Final Study GuidecherokeemNo ratings yet
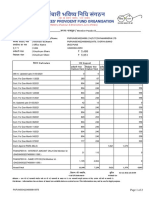
- LNL Iklcqd /: Grand Total 11,109 7,230 5,621 1,379 6,893Document2 pagesLNL Iklcqd /: Grand Total 11,109 7,230 5,621 1,379 6,893Dawood KhanNo ratings yet
- Annotated Bib. Essay PlansDocument6 pagesAnnotated Bib. Essay Planselenutza_dNo ratings yet
- Karakoç 2019bDocument32 pagesKarakoç 2019bAhmet Ali UcarNo ratings yet
- Single ply waterproofing membrane technical data sheetDocument4 pagesSingle ply waterproofing membrane technical data sheetWES QingNo ratings yet
- Philosophers of Antiquity: Confucius Parmenides MoziDocument9 pagesPhilosophers of Antiquity: Confucius Parmenides MoziMaureen Mae EstanolNo ratings yet