You might also like
- Dizziness History and Physical ExaminationDocument30 pagesDizziness History and Physical Examinationrapannika100% (1)
- Janeway's Immunobiology 8thDocument892 pagesJaneway's Immunobiology 8thSergio Falcon Rivera92% (12)
- Apraxia, Agnosia and Disconnection SyndromesDocument65 pagesApraxia, Agnosia and Disconnection SyndromesDhawal Narang100% (1)
- Neuro Assess HandoutDocument14 pagesNeuro Assess HandoutPie ArtWorkNo ratings yet
- Physical Examination Skills Vital for PsychiatristsDocument8 pagesPhysical Examination Skills Vital for PsychiatristsDita Mega UtamiNo ratings yet
- Parietal Lobe TestingDocument5 pagesParietal Lobe TestingvinodksahuNo ratings yet
- Cardiogenic Shock PDFDocument14 pagesCardiogenic Shock PDFAdreiTheTripleANo ratings yet
- Basics of Sleep Architecture and DisordersDocument10 pagesBasics of Sleep Architecture and DisordersQuang VuNo ratings yet
- Sleep PresentationDocument101 pagesSleep Presentationbeauty100% (3)
- Explore the Nervous System in 40 CharactersDocument31 pagesExplore the Nervous System in 40 CharactersDeology JuaninoNo ratings yet
- Physiology of Sleep and ConsciousnessDocument40 pagesPhysiology of Sleep and ConsciousnessZobayer AhmedNo ratings yet
- Motor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistDocument36 pagesMotor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistJim Jose Antony100% (1)
- SMP Neuro Lab ManualDocument37 pagesSMP Neuro Lab Manualsas345sas345No ratings yet
- Neurophysiology, Neurotransmitters and The Nervous SystemDocument69 pagesNeurophysiology, Neurotransmitters and The Nervous SystemKUNNAMPALLIL GEJO JOHN100% (1)
- Cerebellum: Principally Because Electrical Excitation of The CerebellumDocument42 pagesCerebellum: Principally Because Electrical Excitation of The Cerebellumdr_mksinhaNo ratings yet
- Temporal LobeDocument15 pagesTemporal LobeManya KrishnaNo ratings yet
- Heart Failure Mechanisms and Assessment FindingsDocument9 pagesHeart Failure Mechanisms and Assessment Findingssarasmith1988No ratings yet
- Physiology of LiverDocument97 pagesPhysiology of LiverRatna Praveen100% (1)
- Mechanism of HearingDocument203 pagesMechanism of HearingMythily VedhagiriNo ratings yet
- NeurotransmittersDocument39 pagesNeurotransmitterspreetie87No ratings yet
- Acid-Base Regulation and Disorders: Key ConceptsDocument54 pagesAcid-Base Regulation and Disorders: Key ConceptsPaolo Uccello100% (1)
- Exercise ECGDocument85 pagesExercise ECGSUHER ANUNo ratings yet
- Brain Anatomy PDFDocument37 pagesBrain Anatomy PDFPinto D. R PiliangNo ratings yet
- BiofeedbackDocument15 pagesBiofeedbackSofía Esquivel100% (1)
- Posture and EquilibriumDocument26 pagesPosture and Equilibriumshwetha pc100% (1)
- 70 EEG in Focal Epilepsies-Handout PDFDocument70 pages70 EEG in Focal Epilepsies-Handout PDFDragutin PetricNo ratings yet
- Brain Anatomy, Anatomy of The Human BrainDocument12 pagesBrain Anatomy, Anatomy of The Human BrainElmir ƏzimovNo ratings yet
- Evoked PotentialsDocument49 pagesEvoked PotentialsparuNo ratings yet
- Why Non Speech Oral Motor Exercises Are Not WarrantedDocument13 pagesWhy Non Speech Oral Motor Exercises Are Not WarrantedLoreto Opazo RojasNo ratings yet
- AphasiaDocument71 pagesAphasiaVarun B RenukappaNo ratings yet
- Temporal LobeDocument68 pagesTemporal LobeRupinder GillNo ratings yet
- Ascending TractsDocument42 pagesAscending TractsJustine Nyangaresi100% (2)
- Objectives: Pre-Analytical Considerations in PhlebotomyDocument9 pagesObjectives: Pre-Analytical Considerations in PhlebotomyMr. Potatohead100% (1)
- Heart BlockDocument60 pagesHeart Blockmaibejose100% (1)
- Sleep Physiology - DR - EbtehagDocument32 pagesSleep Physiology - DR - EbtehagQairul AzmanNo ratings yet
- Sleep DisordersDocument19 pagesSleep DisordersKaren MogiNo ratings yet
- Eeg Reading TipsDocument6 pagesEeg Reading TipsJULIENo ratings yet
- Elektroencephalogram & Proses Kesadaran: Departemen Fisiologi FK USUDocument21 pagesElektroencephalogram & Proses Kesadaran: Departemen Fisiologi FK USUYohanna SinuhajiNo ratings yet
- AASMRespiratory Events ScoringDocument19 pagesAASMRespiratory Events ScoringAdam GirardoNo ratings yet
- Function Cerebellum Motor ControlDocument38 pagesFunction Cerebellum Motor ControlNaOMi MiNaMiNo ratings yet
- ORLADocument10 pagesORLACarol CoelhoNo ratings yet
- Physiology of Sleep: Unconsciousness From Which The Person Can Be Aroused by Sensory or Other StimuliDocument8 pagesPhysiology of Sleep: Unconsciousness From Which The Person Can Be Aroused by Sensory or Other StimulibnmjgcNo ratings yet
- Jugular Venous PressureDocument9 pagesJugular Venous Pressuremoh86-No ratings yet
- Physiology of SleepDocument26 pagesPhysiology of SleepDuiiiiNo ratings yet
- Sleep and ExerciseDocument14 pagesSleep and ExerciseAhmad YasinNo ratings yet
- CNS - Limbic SystemDocument46 pagesCNS - Limbic SystemsarvinaNo ratings yet
- Aphasia, Apraxia, and Agnosia AphasiaDocument7 pagesAphasia, Apraxia, and Agnosia Aphasiasomebody_maNo ratings yet
- Aphasia 07Document34 pagesAphasia 07razik89No ratings yet
- Automated Scoring of A Neuropsychological Test The Rey OsterrietDocument8 pagesAutomated Scoring of A Neuropsychological Test The Rey OsterrietMilosNo ratings yet
- 1533 The Dysphagia Toolbox Validated Assessment Tools For Dysphagia in AdultsDocument33 pages1533 The Dysphagia Toolbox Validated Assessment Tools For Dysphagia in AdultsAlvaro Martinez TorresNo ratings yet
- Physiology Review: Neurophysiology: (Based On Guyton's and Personal Extras)Document5 pagesPhysiology Review: Neurophysiology: (Based On Guyton's and Personal Extras)djxela89No ratings yet
- Anatomical Positions and Terminology GuideDocument127 pagesAnatomical Positions and Terminology GuideMaria JozilynNo ratings yet
- Neuroplasticity in AphasiaDocument10 pagesNeuroplasticity in AphasiaCoti Canales YoshidzumiNo ratings yet
- Human AnatomyDocument265 pagesHuman AnatomynicevenuNo ratings yet
- Brain Injury and Epilepsy: What Is An Epileptic Seizure?Document4 pagesBrain Injury and Epilepsy: What Is An Epileptic Seizure?kaninerNo ratings yet
- Respiratory System WorksheetDocument2 pagesRespiratory System WorksheetPeter Mazowiecki-KocykNo ratings yet
- BiofeedbackDocument5 pagesBiofeedbackJasmine KashyapNo ratings yet
- Sleep DisordersDocument588 pagesSleep DisordersDavid SmithNo ratings yet
- Aca - 1Document28 pagesAca - 1Aparna LVNo ratings yet
- Electrical Activity of the Brain, Sleep–Wake States, & Circadian Rhythms (BMS1-K4Document26 pagesElectrical Activity of the Brain, Sleep–Wake States, & Circadian Rhythms (BMS1-K4Zikri Putra Lan LubisNo ratings yet
- EEG and SLEEPDocument25 pagesEEG and SLEEPAditya SahNo ratings yet
- Pertemuan 14 Consciousness 2122Document22 pagesPertemuan 14 Consciousness 2122Azizah RatnaNo ratings yet
- Sleep: Ty Lees School of Life SciencesDocument25 pagesSleep: Ty Lees School of Life SciencesMawj MandwieNo ratings yet
- Chapter 9 Fact SheetDocument4 pagesChapter 9 Fact SheetJustynmae JusainNo ratings yet
- Hafizah Binti Mohd Hoshni Sleep & Alert BehaviourDocument39 pagesHafizah Binti Mohd Hoshni Sleep & Alert BehaviourHafizah HoshniNo ratings yet
- Consciousness: # IntroDocument7 pagesConsciousness: # IntroDaizy DharewalNo ratings yet
- How Prolonged Immobilization Negatively Impacts the BodyDocument45 pagesHow Prolonged Immobilization Negatively Impacts the BodyjhnaidillaNo ratings yet
- Lymphatic SystemDocument2 pagesLymphatic Systemmeg leeNo ratings yet
- Ms - CardiovascularDocument70 pagesMs - CardiovascularMark OngNo ratings yet
- Wearable and Implantable Sensors For Biomedical ApplicationsDocument22 pagesWearable and Implantable Sensors For Biomedical ApplicationsEsteban MuñozNo ratings yet
- Literature Review 1Document4 pagesLiterature Review 1api-534394198No ratings yet
- MS Cardio Lecture EDITEDDDocument28 pagesMS Cardio Lecture EDITEDDsanchezanya34No ratings yet
- PhotosynthesisDocument4 pagesPhotosynthesisRishar bokNo ratings yet
- 21 BurnsDocument16 pages21 BurnsPriyaNo ratings yet
- 2nd Pharmacology Sessional PaperDocument2 pages2nd Pharmacology Sessional PaperRaman NaiknawareNo ratings yet
- Chapter 42 Circulation and Gas ExchangeDocument16 pagesChapter 42 Circulation and Gas ExchangeBeck MicksNo ratings yet
- High school drug rehabilitation case studiesDocument3 pagesHigh school drug rehabilitation case studiesAudrie Allyson GabalesNo ratings yet
- Common Ecg Abnormalities PDFDocument2 pagesCommon Ecg Abnormalities PDFRonNo ratings yet
- George K. Aghajanian and Elaine Sanders-Bush - SerotoninDocument20 pagesGeorge K. Aghajanian and Elaine Sanders-Bush - SerotoninSour60No ratings yet
- 8.1 - Nervous Impulses - 1Document8 pages8.1 - Nervous Impulses - 1jamilNo ratings yet
- NUR1101 - Endocrine System Functions and Control MechanismsDocument6 pagesNUR1101 - Endocrine System Functions and Control MechanismsJohnNo ratings yet
- Unit 1Document3 pagesUnit 1Omaiwa Mo ShinderuNo ratings yet
- Cardiorespiratory Endurance: in This Chapter Student Web ResourcesDocument9 pagesCardiorespiratory Endurance: in This Chapter Student Web ResourcesFRANCO PANUGALINGNo ratings yet
- Sleep DisordersDocument45 pagesSleep DisordersOse IbhadodeNo ratings yet
- 1153-Article Text-4888-1-10-20200206 PDFDocument6 pages1153-Article Text-4888-1-10-20200206 PDFAdrian CaballesNo ratings yet
- BERNARDI Slow BreathingDocument68 pagesBERNARDI Slow BreathingMiklós BalatinczNo ratings yet
- PIIS0896627316310078Document27 pagesPIIS0896627316310078Carolina RicárdezNo ratings yet
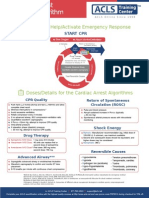
- Shout For Help/Activate Emergency Response: CPR StartDocument2 pagesShout For Help/Activate Emergency Response: CPR StartdavpierNo ratings yet
- NURSING-CARE-PLAN With AnswersDocument4 pagesNURSING-CARE-PLAN With AnswersTracy Malingin QuimqueNo ratings yet
- Dressler's Syndrome Case ReportDocument3 pagesDressler's Syndrome Case ReportResearch ParkNo ratings yet