You might also like
- Approach To The Diagnosis of Heart Diseases 2Document61 pagesApproach To The Diagnosis of Heart Diseases 2Patricia VirginiaNo ratings yet
- What's New in Respiratory DisordersDocument4 pagesWhat's New in Respiratory DisorderssobanNo ratings yet
- CPG Management of Hypertension 4th EditionDocument98 pagesCPG Management of Hypertension 4th EditionPervinder SinghNo ratings yet
- Resistant Hypertension. AHADocument38 pagesResistant Hypertension. AHAEderEmmanuelMartinezRuiz100% (1)
- Pharmacovigilance DefinationsDocument32 pagesPharmacovigilance DefinationsKadir AmirNo ratings yet
- Preventive CardiologyDocument28 pagesPreventive CardiologyerizonNo ratings yet
- WHO MDR 2020 Handbook Treatment PDFDocument88 pagesWHO MDR 2020 Handbook Treatment PDFYuanita GunawanNo ratings yet
- Dengue DiagnosisDocument160 pagesDengue DiagnosisBayu Cahyo OktafianNo ratings yet
- Mitral Valve Prolapse, Flailed Mitral Valve Mitral Annular CalcificationDocument33 pagesMitral Valve Prolapse, Flailed Mitral Valve Mitral Annular CalcificationcafemedNo ratings yet
- Acute Incisional Hernia: Theme From September 2011 ExamDocument146 pagesAcute Incisional Hernia: Theme From September 2011 ExamVimal Kumar YadavNo ratings yet
- HIV-associated Nephropathy (HIVAN) - UpToDate PDFDocument22 pagesHIV-associated Nephropathy (HIVAN) - UpToDate PDFMuh Deriyatmiko BastamanNo ratings yet
- What Is Being Tested?: White Blood CellsDocument48 pagesWhat Is Being Tested?: White Blood Cellsstudent_019No ratings yet
- 2019 - MCardiology - Clinical Features of Val HT 2019 2Document72 pages2019 - MCardiology - Clinical Features of Val HT 2019 2Vaenusha MuruganNo ratings yet
- Heart MurmursDocument16 pagesHeart MurmursPriyam SinghNo ratings yet
- NEJM Treatment of Patients With Cirrohsis Aug 2016Document11 pagesNEJM Treatment of Patients With Cirrohsis Aug 2016risewfNo ratings yet
- Diseases of The CvsDocument24 pagesDiseases of The CvsHussein Al SaediNo ratings yet
- 09.cutaneous Manifestations of Systemic DiseasesDocument51 pages09.cutaneous Manifestations of Systemic DiseasesMohamed Rikarz Ahamed RikarzNo ratings yet
- Key Board Short CutDocument6 pagesKey Board Short CutChaitanya KumarNo ratings yet
- 5 - Endocrinology Passmedicine Q. Bank PART I 2017Document366 pages5 - Endocrinology Passmedicine Q. Bank PART I 2017'محمد علي' محمد لافي100% (1)
- PedsnotesDocument18 pagesPedsnoteskp13oyNo ratings yet
- Mis C Clinical GuidelineDocument9 pagesMis C Clinical GuidelineasyqarNo ratings yet
- Carbohydrate Metabolism Disorders Stom 10-11Document61 pagesCarbohydrate Metabolism Disorders Stom 10-11Artem GrigoryanNo ratings yet
- Solitary Nodule of Thyroid DR.B.VDocument18 pagesSolitary Nodule of Thyroid DR.B.VpranapushpaNo ratings yet
- History and Physical Examination TemplateDocument3 pagesHistory and Physical Examination TemplateRawa MuhsinNo ratings yet
- IV Infusion: Purpose of Starting IV'sDocument6 pagesIV Infusion: Purpose of Starting IV'sKiara Denise TamayoNo ratings yet
- Classification of The DrugsDocument50 pagesClassification of The DrugsGlena SalamNo ratings yet
- Opthalmology NotesDocument39 pagesOpthalmology NotesjerinthomasrajanNo ratings yet
- Valvular Heart Disease. KulDocument60 pagesValvular Heart Disease. KulIntan Kumalasari RambeNo ratings yet
- Part 1 EP ClinicalDocument28 pagesPart 1 EP ClinicalHany100% (2)
- Ischemic Heart Disease 19.9.90Document27 pagesIschemic Heart Disease 19.9.90Hamidreza GoodarzynejadNo ratings yet
- The Quest For New Approaches in Myocarditis and in Ammatory CardiomyopathyDocument18 pagesThe Quest For New Approaches in Myocarditis and in Ammatory Cardiomyopathyrohman cooyNo ratings yet
- Clinical ExDocument123 pagesClinical ExDeepti ChaharNo ratings yet
- AnaemiaDocument71 pagesAnaemiaREETHUNo ratings yet
- Usmle RX Qbank 2017 Step 1 Cardiology PhysiologyDocument117 pagesUsmle RX Qbank 2017 Step 1 Cardiology PhysiologySreeNo ratings yet
- Acute Abdominal Pain: Presented by Dr. Kolahdouzan Thoracic Surgen Alzahra HospitalDocument77 pagesAcute Abdominal Pain: Presented by Dr. Kolahdouzan Thoracic Surgen Alzahra HospitalGraceline Margaretha Marsintauly SianiparNo ratings yet
- Daily Duas in The Month ofDocument258 pagesDaily Duas in The Month ofTransforNo ratings yet
- Pericarditis 65 SlidesDocument65 pagesPericarditis 65 SlidesAtifBhoreNo ratings yet
- Vascular Overview May 2009Document60 pagesVascular Overview May 2009BryndenNo ratings yet
- Crdiology - DR Abo-ElAsrar - by El Azhar Medical Students 2012Document74 pagesCrdiology - DR Abo-ElAsrar - by El Azhar Medical Students 2012Raouf Ra'fat SolimanNo ratings yet
- DVTDocument13 pagesDVTapi-253732526No ratings yet
- Step 2ck Important (AutoRecovered)Document101 pagesStep 2ck Important (AutoRecovered)Aishwarya SridharNo ratings yet
- Young Stroke Etiology and Clinical ApproachDocument43 pagesYoung Stroke Etiology and Clinical ApproachDr Prakash HarischandraNo ratings yet
- Cardiovascular Medicine:Question 1Document101 pagesCardiovascular Medicine:Question 1abdullahmushlihNo ratings yet
- WeitzmanDocument5 pagesWeitzmandanielmoffatNo ratings yet
- 14) PPT ROMAN Salah Training - StudentsDocument342 pages14) PPT ROMAN Salah Training - Studentsamer sohailNo ratings yet
- SyncopeDocument3 pagesSyncopeanishdNo ratings yet
- Part 2 Exam Sample Q 2015Document194 pagesPart 2 Exam Sample Q 2015Abdul QuyyumNo ratings yet
- Parathyroid Disease Lecture SlidesDocument50 pagesParathyroid Disease Lecture SlidesMaxwell PalSingh100% (1)
- Clinical Science Section Acute Abdomen: Preseptor: Dr. Liza Nursanty, SPB, Mkes, FinacsDocument40 pagesClinical Science Section Acute Abdomen: Preseptor: Dr. Liza Nursanty, SPB, Mkes, FinacsPraluki HerliawanNo ratings yet
- FcpsDocument206 pagesFcpsDRwaqas GulzarNo ratings yet
- HivDocument36 pagesHivfenendriyaniNo ratings yet
- Prevention of DVT/PE: Noornadia BT Yahaya 050100841Document32 pagesPrevention of DVT/PE: Noornadia BT Yahaya 050100841Nadia YahayaNo ratings yet
- 10.08.07 Cardiac Tamponade HaagDocument16 pages10.08.07 Cardiac Tamponade HaagfoetorNo ratings yet
- Cardiomyopathy: Dr. Ibrahim AbuasbehDocument39 pagesCardiomyopathy: Dr. Ibrahim Abuasbehأبوأحمد الحكيمNo ratings yet
- Basic Arrythmia AnalysisDocument60 pagesBasic Arrythmia AnalysisZakky KurniawanNo ratings yet
- OSCE Internal MedicineDocument4 pagesOSCE Internal Medicinemohamed mowafeyNo ratings yet
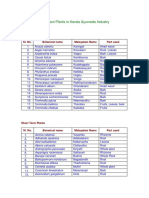
- Important Plants in Kerala Ayurveda Industry: Tree CropsDocument2 pagesImportant Plants in Kerala Ayurveda Industry: Tree Cropsajeez86No ratings yet
- Confused: Get Composed and Confident!Document4 pagesConfused: Get Composed and Confident!Muhammad Tariq KhanNo ratings yet
- SālsLetterV3 2 PDFDocument8 pagesSālsLetterV3 2 PDFMuhammad Tariq KhanNo ratings yet
- SālsLetterV3 1 PDFDocument8 pagesSālsLetterV3 1 PDFMuhammad Tariq KhanNo ratings yet
- SālsLetterV3 4to6 PDFDocument8 pagesSālsLetterV3 4to6 PDFMuhammad Tariq KhanNo ratings yet
- SālsLetterV3 3 PDFDocument8 pagesSālsLetterV3 3 PDFMuhammad Tariq KhanNo ratings yet
- PharmaDocument2 pagesPharmaMuhammad Tariq KhanNo ratings yet
- Self Study Quiz With Answer SheetDocument6 pagesSelf Study Quiz With Answer SheetHuma Hameed DogarNo ratings yet
- Antimycobacterial Drugs MuddassirDocument66 pagesAntimycobacterial Drugs MuddassirMuhammad Tariq KhanNo ratings yet
- ImportantDocument11 pagesImportantMuhammad Tariq KhanNo ratings yet
- Marketing Tariq Khan For RWPDocument2 pagesMarketing Tariq Khan For RWPMuhammad Tariq KhanNo ratings yet
- The Human Circulatory System by TariqDocument84 pagesThe Human Circulatory System by TariqMuhammad Tariq KhanNo ratings yet
- Very Imp.045Document13 pagesVery Imp.045Muhammad Tariq KhanNo ratings yet
- AlamgirDocument7 pagesAlamgirMuhammad Tariq KhanNo ratings yet
- 45 SharmaDocument14 pages45 SharmaMuhammad Tariq KhanNo ratings yet
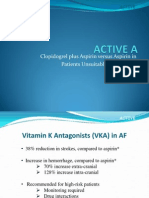
- Clopidogrel Plus Aspirin Versus Aspirin in Patients Unsuitable For WarfarinDocument22 pagesClopidogrel Plus Aspirin Versus Aspirin in Patients Unsuitable For WarfarinMuhammad Tariq KhanNo ratings yet
- Alamgeer 2bbnnDocument6 pagesAlamgeer 2bbnnMuhammad Tariq KhanNo ratings yet
- The Primary and Secondary Prevention of Cardiovascular DiseaseDocument20 pagesThe Primary and Secondary Prevention of Cardiovascular DiseaseMuhammad Tariq KhanNo ratings yet
- Acetylsalicylic AcidDocument13 pagesAcetylsalicylic AcidMuhammad Tariq Khan100% (1)
- License Snadav Logo Adalah Daftar Pengunaan Smadav Selama Pemakaian.Document5 pagesLicense Snadav Logo Adalah Daftar Pengunaan Smadav Selama Pemakaian.Vika PipianiNo ratings yet
- Arterial UlcersDocument8 pagesArterial Ulcerspka25No ratings yet
- Peripheral Vascular Disease - WL GanDocument2 pagesPeripheral Vascular Disease - WL GanWeh Loong Gan100% (1)
- Critical Limb IschemiaDocument2 pagesCritical Limb IschemiaDorin DvornicNo ratings yet
- Burger Allen Exercises pdf1Document133 pagesBurger Allen Exercises pdf1lucky 116No ratings yet
- Peripheral Arterial DiseaseDocument11 pagesPeripheral Arterial DiseaseAnas YahyaNo ratings yet
- 4 Mezil & Abed, 2021 Review - Complication of Diabetes MellitusDocument12 pages4 Mezil & Abed, 2021 Review - Complication of Diabetes Mellitusbangd1f4nNo ratings yet
- Stroke Related Thesis TopicsDocument6 pagesStroke Related Thesis Topicskatrekahowardatlanta100% (2)
- Vascular Vascular: Medicine (ST George's Hospital Medical School) Medicine (ST George's Hospital Medical School)Document7 pagesVascular Vascular: Medicine (ST George's Hospital Medical School) Medicine (ST George's Hospital Medical School)shravaniNo ratings yet
- MedCosmos Surgery - History TakingDocument18 pagesMedCosmos Surgery - History TakingEmmanuel DanielsNo ratings yet
- Cardio Exam Test BankDocument17 pagesCardio Exam Test BankPINKY CUARESMA0% (1)
- Iwgdf 2023 02Document38 pagesIwgdf 2023 02Luis Carlos de CáceresNo ratings yet
- Appendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexDocument26 pagesAppendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexabigailNo ratings yet
- Diabetes in The UK 2010Document21 pagesDiabetes in The UK 2010jrjsdNo ratings yet
- A Detailed Lesson Plan in Living ThingsDocument23 pagesA Detailed Lesson Plan in Living ThingsclarisseNo ratings yet
- Endovascular Solution in Peripheral Artery DiseaseDocument36 pagesEndovascular Solution in Peripheral Artery DiseaseArintia AubreyNo ratings yet
- 201501119jackwin Sam PaulDocument138 pages201501119jackwin Sam PaulSanjivi GovekarNo ratings yet
- Diabetic Foot Ulcer - Prameha PidikaDocument28 pagesDiabetic Foot Ulcer - Prameha PidikaPayal SindelNo ratings yet
- SHENAAZ Surgical Chronicles - Final VersionDocument6 pagesSHENAAZ Surgical Chronicles - Final VersionSumayyah EbrahimNo ratings yet
- (Traves D. Crabtree) BRS Surgical Specialties PDFDocument254 pages(Traves D. Crabtree) BRS Surgical Specialties PDFCosmin Alexa100% (2)
- Diabetic Foot: The Orthopedic Surgery Angle:, T. Leemrijse, P.-A. DeleuDocument16 pagesDiabetic Foot: The Orthopedic Surgery Angle:, T. Leemrijse, P.-A. DeleuDewi Sartika100% (1)
- Step 2 Guide PDFDocument87 pagesStep 2 Guide PDFAlan Ahlawat SumskiNo ratings yet
- Ankle-Brachial Index For Assessment of Peripheral Arterial DiseaseDocument5 pagesAnkle-Brachial Index For Assessment of Peripheral Arterial DiseaseindrawepeNo ratings yet
- Common Drugs With Effective Off-Label UsesDocument10 pagesCommon Drugs With Effective Off-Label Usesredwan_rnNo ratings yet
- A Detailed Lesson Plan in Living Things and Their Environment (Respiratory and Circulatory System: Relation)Document22 pagesA Detailed Lesson Plan in Living Things and Their Environment (Respiratory and Circulatory System: Relation)Don LaguismaNo ratings yet
- Cardiovascular System: AnatomyDocument19 pagesCardiovascular System: AnatomyStephanie MacVeighNo ratings yet
- Acute Arterial OcclusionDocument58 pagesAcute Arterial Occlusioneb3tleNo ratings yet
- Assessment of The Peripheral Vascular SystemDocument91 pagesAssessment of The Peripheral Vascular SystemKeid Reuma100% (1)
- Core Curriculum For NursesDocument17 pagesCore Curriculum For NursesRaden Roro Atih Utari RizkyNo ratings yet
- Delayed Diagnosis of Ischemia After Popliteal Artery Injury During Total Knee ArthroplastyDocument4 pagesDelayed Diagnosis of Ischemia After Popliteal Artery Injury During Total Knee ArthroplastyHerald Scholarly Open AccessNo ratings yet
- Peripheral Arterial DseDocument2 pagesPeripheral Arterial Dsemiss RNNo ratings yet