You might also like
- Tata Laksana Sindroma Koroner Akut: Cholid Tri TjahjonoDocument84 pagesTata Laksana Sindroma Koroner Akut: Cholid Tri TjahjonoVio Alveolita PrimayaniNo ratings yet
- CURRICULUM VITAE OF DENGUE EXPERTDocument59 pagesCURRICULUM VITAE OF DENGUE EXPERTsaladass 2No ratings yet
- KEYNOTE UKMPPD "NEURODocument20 pagesKEYNOTE UKMPPD "NEUROfardan chaisarNo ratings yet
- Acute Coronary Syndrome 052014Document91 pagesAcute Coronary Syndrome 052014Fatahillah NazarNo ratings yet
- PPDS - AR - 22 16 - Agu - P Ilovepdf Compressed Ilovepdf C PDFDocument192 pagesPPDS - AR - 22 16 - Agu - P Ilovepdf Compressed Ilovepdf C PDFlaboratorium rshmdn100% (1)
- Kuliah ADENOMYOSISDocument38 pagesKuliah ADENOMYOSISmarajuuNo ratings yet
- Thyroid DiseasesDocument76 pagesThyroid DiseasesSolomon Fallah Foa SandyNo ratings yet
- Kumpulan POMRDocument26 pagesKumpulan POMRIMN Wiranta PrasetyajiNo ratings yet
- TiroidDocument26 pagesTiroidJoni Riana MustaqimNo ratings yet
- Tehnik Balut MembalutDocument24 pagesTehnik Balut MembalutmelisandrianaNo ratings yet
- Timing Issues in Fracture Management: A Review of Current ConceptsDocument9 pagesTiming Issues in Fracture Management: A Review of Current ConceptsRizka Nurul FirdausNo ratings yet
- Interna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityDocument46 pagesInterna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityErni JawaNo ratings yet
- KARDIOMYOPATI: Understanding Heart Muscle DiseasesDocument28 pagesKARDIOMYOPATI: Understanding Heart Muscle DiseasesArif Zulfian MubarokNo ratings yet
- Askep MCI - AchirmanDocument53 pagesAskep MCI - AchirmanmarthaNo ratings yet
- Kuliah Periodic Paralysis Akibat TirotoksikosisDocument14 pagesKuliah Periodic Paralysis Akibat TirotoksikosisFarnida JamhalNo ratings yet
- Pembahasan TO 3 Agustus 15 PDFDocument802 pagesPembahasan TO 3 Agustus 15 PDFFahmi Afif AlbonehNo ratings yet
- Referat DHF DoraDocument23 pagesReferat DHF Dorareza prayogaNo ratings yet
- Kul Sem 4 Heat Stroke N Fever UHT 2016Document63 pagesKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaNo ratings yet
- Cerebral Toxoplasmosis: Diagnosis & ManagementDocument32 pagesCerebral Toxoplasmosis: Diagnosis & ManagementShinta DianNo ratings yet
- 1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018Document46 pages1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018ดนุ เกษรศิริNo ratings yet
- Daftar Kode Diagnosa & TindakanDocument7 pagesDaftar Kode Diagnosa & Tindakannovi andriyaniNo ratings yet
- Panthea v29 Short WalkthroughDocument1 pagePanthea v29 Short WalkthroughHenrique Mendes GewehrNo ratings yet
- Case Report Kejang DemamDocument48 pagesCase Report Kejang DemamRahmatNo ratings yet
- Ocular Examination & InvestigationDocument17 pagesOcular Examination & Investigationapi-3698227100% (1)
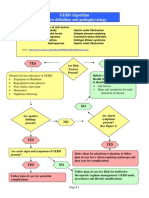
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocument3 pagesGERD Algorithm Review Definition and Pathophysiology: NO YESdianyNo ratings yet
- Thalassemia PresentationDocument9 pagesThalassemia Presentationapi-278076677No ratings yet
- Death Case Dr. MeikoDocument49 pagesDeath Case Dr. MeikoMohamad ZulfikarNo ratings yet
- Assessment and Initial Management Trauma PatientDocument69 pagesAssessment and Initial Management Trauma PatientdrpagrawNo ratings yet
- Understanding NystagmusDocument14 pagesUnderstanding NystagmusJefferson CaesarioNo ratings yet
- IPDIDocument30 pagesIPDIaris budionoNo ratings yet
- Larynx InfectionsDocument28 pagesLarynx InfectionsMuskan GogiaNo ratings yet
- Referat HDKDocument29 pagesReferat HDKAga Haris100% (1)
- AcdDocument14 pagesAcdSamsul BahriNo ratings yet
- Lecture 15-Autoimmune Disease of The Skin-Hardyanto Soebono (2017)Document58 pagesLecture 15-Autoimmune Disease of The Skin-Hardyanto Soebono (2017)Alfina MeidinaNo ratings yet
- Informed Consent Forensik KlinikDocument3 pagesInformed Consent Forensik KlinikAnggita Efipania Silambi'No ratings yet
- Diagnosis Dan Tatalaksana Syok Di Layanan Primer: Rs Pratama Teluk KeramatDocument45 pagesDiagnosis Dan Tatalaksana Syok Di Layanan Primer: Rs Pratama Teluk KeramatNight BaronNo ratings yet
- OsteoarthritisDocument29 pagesOsteoarthritisfizhazhiNo ratings yet
- Pain Dan Kaku Leher Akibat Capsular Pattern Kasus SACDocument10 pagesPain Dan Kaku Leher Akibat Capsular Pattern Kasus SACAfifah NurNo ratings yet
- Thyroid DiseaseDocument17 pagesThyroid DiseaseCharlz ZipaganNo ratings yet
- PAT + Primary SurveyDocument33 pagesPAT + Primary Surveysalsa100% (1)
- Sindrom Nefrotik: Disusun Oleh: Wijdani SharfinaDocument34 pagesSindrom Nefrotik: Disusun Oleh: Wijdani Sharfinasharfina21No ratings yet
- Morning Report: 4yo Girl With Bloody DiarrheaDocument18 pagesMorning Report: 4yo Girl With Bloody DiarrheaVanny FolandaNo ratings yet
- Management of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientDocument12 pagesManagement of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientRani Dwi NNo ratings yet
- There Are Safe Methods To Prevent Pregnancy After Unprotected SexDocument8 pagesThere Are Safe Methods To Prevent Pregnancy After Unprotected SexAnjaliSinhaNo ratings yet
- Anemia E.C Hematemesis Melena E.C Suspect Gastritis ErrosiveDocument37 pagesAnemia E.C Hematemesis Melena E.C Suspect Gastritis ErrosiveAndayanaIdhamNo ratings yet
- Teori Obat DispepsiaDocument13 pagesTeori Obat DispepsiaPasti SuksesNo ratings yet
- Autoimmune Hemolytic AnaemiaDocument32 pagesAutoimmune Hemolytic AnaemiaJohn VinithNo ratings yet
- Auto Immune Hemolytic Anemia: Dr. Devesh A. Tiwari Pediatric Hematology Oncology LTMMC & GHDocument37 pagesAuto Immune Hemolytic Anemia: Dr. Devesh A. Tiwari Pediatric Hematology Oncology LTMMC & GHdrdeveshNo ratings yet
- Hemolytic AnemiaDocument43 pagesHemolytic AnemiaDudi100% (5)
- Autoimmune Hemolytic AnemiaDocument17 pagesAutoimmune Hemolytic AnemiaIrina IordachescuNo ratings yet
- Acquired Hemolytic Anemia Presentation For BPharmDocument24 pagesAcquired Hemolytic Anemia Presentation For BPharmHiren Pathak100% (2)
- What Is Destroying This RBC?Document28 pagesWhat Is Destroying This RBC?Putri Azka RinandaNo ratings yet
- 13 Other Blood Group SystemsDocument56 pages13 Other Blood Group SystemsCarinaJongLeeNo ratings yet
- Compiled By:: G.A.R. Sampath Kalhari Gihara Chanaka Lakshan Aqeela ManuideenDocument28 pagesCompiled By:: G.A.R. Sampath Kalhari Gihara Chanaka Lakshan Aqeela ManuideenYashvanth YashNo ratings yet
- Anemia HemolitikDocument83 pagesAnemia HemolitikWinda A. PanjaitanNo ratings yet
- Coombs-test-HDNDocument46 pagesCoombs-test-HDNbchinmay123456No ratings yet
- Anemia Hemolytic - Dr. MulatDocument83 pagesAnemia Hemolytic - Dr. MulatbolabundarNo ratings yet
- Hemolytic AnemiaDocument60 pagesHemolytic AnemiaReta megersaNo ratings yet
- Immuno HematologyDocument24 pagesImmuno HematologyHoraa H AL-marhoonNo ratings yet
- Chapter 25 - Extrinsic Defects Leading To Increased Erythrocyte Destruction - Immune Causes Final DraftDocument2 pagesChapter 25 - Extrinsic Defects Leading To Increased Erythrocyte Destruction - Immune Causes Final DraftNathaniel SimNo ratings yet
- Li CHFDocument27 pagesLi CHFRandy GipsonNo ratings yet
- The Risk Factors of Nutritional Disorders To The Cardiovascular SystemDocument6 pagesThe Risk Factors of Nutritional Disorders To The Cardiovascular SystemFitriani LastariNo ratings yet
- Anemia Hemolitik Pada AnakDocument22 pagesAnemia Hemolitik Pada AnakRandy GipsonNo ratings yet
- Nutritional AnemiaDocument6 pagesNutritional AnemiaRandy GipsonNo ratings yet
- Diseases of Lymph Nodes 5Document32 pagesDiseases of Lymph Nodes 5barendyanoNo ratings yet
- AnaphylaxisDocument36 pagesAnaphylaxisRamdan Dani MuslihatNo ratings yet
- Disorders of Lymphatic SystemDocument43 pagesDisorders of Lymphatic SystemNurfanida Natasya MNo ratings yet
- Rhinitis AlergiDocument35 pagesRhinitis AlergiRandy GipsonNo ratings yet
- Alergi ObatDocument20 pagesAlergi ObatRandy GipsonNo ratings yet
- Hellp SyndromeDocument5 pagesHellp SyndromeJmarie Brillantes PopiocoNo ratings yet
- Minor Blood Groups Part 1Document15 pagesMinor Blood Groups Part 1Mary Shikha ShaikeNo ratings yet
- Kidd Blood Group System (2Document4 pagesKidd Blood Group System (2RSH1987100% (1)
- Nursing Care of The Family Experiencing A Sudden Pregnancy ComplicationDocument7 pagesNursing Care of The Family Experiencing A Sudden Pregnancy ComplicationDacillo GailleNo ratings yet
- Blood Banking Progress ExamDocument67 pagesBlood Banking Progress ExamlenvycahpdelusaNo ratings yet
- 10 11648 J Ijgg 20150301 12jshshahDocument12 pages10 11648 J Ijgg 20150301 12jshshahDiki MartikaNo ratings yet
- High Risk NewbornDocument4 pagesHigh Risk NewbornWenn Joyrenz ManeclangNo ratings yet
- Complement Fixation TestDocument2 pagesComplement Fixation TestGIST (Gujarat Institute of Science & Technology)100% (1)
- Essentials of Human Diseases and Conditions 6th Edition Frazier Test BankDocument25 pagesEssentials of Human Diseases and Conditions 6th Edition Frazier Test BankDavidWilliamsxwdgs100% (13)
- Blood Group System - EssayDocument9 pagesBlood Group System - EssayMarleth100% (1)
- Blood Disorders Seminar No 7Document142 pagesBlood Disorders Seminar No 7Hysum Mushtaq100% (1)
- Hematological Disorders of NewbornDocument98 pagesHematological Disorders of Newbornlieynna499650% (2)
- Anatomy and Physiology 2 Lab ManualDocument129 pagesAnatomy and Physiology 2 Lab ManualMAJEETH மஜீத் TIRUNELVELINo ratings yet
- Hemolytic Disease of The Fetus and NewbornDocument6 pagesHemolytic Disease of The Fetus and NewbornCj CCNo ratings yet
- ImmunohematologyDocument11 pagesImmunohematologydtimtimanNo ratings yet
- Module Answers 1 60 MCN 2Document151 pagesModule Answers 1 60 MCN 2bekbekk cabahug100% (6)
- AUBF Amniotic FluidDocument6 pagesAUBF Amniotic FluidRichelyn Grace B. VenusNo ratings yet
- Voxs 12593Document28 pagesVoxs 12593Arifani CahyaniNo ratings yet
- Heme Synthesis Breakdown HBDocument18 pagesHeme Synthesis Breakdown HBDr.P.NatarajanNo ratings yet
- Anatomy and Physiology 2 Lab Manual 1616118382Document107 pagesAnatomy and Physiology 2 Lab Manual 1616118382Chu NamNo ratings yet
- Hemolytic AnemiaDocument43 pagesHemolytic AnemiaDudi100% (5)
- Blood Groups Practical NewDocument19 pagesBlood Groups Practical NewSreedeep TejaNo ratings yet
- Blood BiochemistryDocument124 pagesBlood BiochemistrySohail AhamdNo ratings yet
- Normocytic Normochromic AnemiaDocument18 pagesNormocytic Normochromic AnemiaElaizha PagulayanNo ratings yet
- Blood Groups SystemsDocument7 pagesBlood Groups SystemsMir jaliesNo ratings yet
- Understanding Blood Disorders: An Overview of Anemia and LeukemiaDocument96 pagesUnderstanding Blood Disorders: An Overview of Anemia and LeukemiaIndragee EkanayakeNo ratings yet
- Nucama 350Document17 pagesNucama 350BFKHONo ratings yet
- Nursing Care Plan JaundiceDocument24 pagesNursing Care Plan Jaundicegandhialpit76% (29)
- Kell and Kidd Blood Group SystemsDocument4 pagesKell and Kidd Blood Group SystemsMaria Chacón CarbajalNo ratings yet
- Matrix Board Exam - MedtechDocument6 pagesMatrix Board Exam - MedtechCaptain MarvelNo ratings yet