You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Health and Caregiving Workforce: An Array of InequitiesDocument16 pagesThe Health and Caregiving Workforce: An Array of InequitiesPresentaciones_FKNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Innovations in Breast Cancer TreatmentDocument21 pagesInnovations in Breast Cancer TreatmentPresentaciones_FKNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Closing The Cancer Divide & Strengthening Health Systems: Interwoven OpportunitiesDocument39 pagesClosing The Cancer Divide & Strengthening Health Systems: Interwoven OpportunitiesPresentaciones_FKNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Closing The Global Pain Divide: An Equity and Health ImperativeDocument16 pagesClosing The Global Pain Divide: An Equity and Health ImperativePresentaciones_FKNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Unpaid Health Care and Caregiving: A Gendered and Hidden Yet Indispensable Subsidy To Economic and Social Development.Document16 pagesUnpaid Health Care and Caregiving: A Gendered and Hidden Yet Indispensable Subsidy To Economic and Social Development.Presentaciones_FKNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Breast Cancer in The Americas: Closing Divides Through Systemic Innovation & AdvocacyDocument33 pagesBreast Cancer in The Americas: Closing Divides Through Systemic Innovation & AdvocacyPresentaciones_FKNo ratings yet
- Breast Cancer Disparities: Closing Global DividesDocument37 pagesBreast Cancer Disparities: Closing Global DividesPresentaciones_FKNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Closing Cancer Divided: Expanding Access To Care & ControlDocument46 pagesClosing Cancer Divided: Expanding Access To Care & ControlPresentaciones_FKNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Breast Cancer in The AmericasDocument27 pagesBreast Cancer in The AmericasPresentaciones_FKNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- La Mujer Ante El COVID-19: Retos y Oportunidades para La Salud y El Sector Salud.Document36 pagesLa Mujer Ante El COVID-19: Retos y Oportunidades para La Salud y El Sector Salud.Presentaciones_FKNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Alleviating The Access Abyss in Palliative Care and Pain Relief.Document37 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief.Presentaciones_FKNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Closing The Divide in Access To Palliative Care and Pain ReliefDocument45 pagesClosing The Divide in Access To Palliative Care and Pain ReliefPresentaciones_FKNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Alleviating The Access Abyss in Palliative Care and Pain Relief: An Imperative of Universal Health CoverageDocument36 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief: An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument44 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument19 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Closing Cancer Divided: Expanding Access To Care & ControlDocument41 pagesClosing Cancer Divided: Expanding Access To Care & ControlPresentaciones_FKNo ratings yet
- Evidence-Inspired Advocacy and Advocacy-Based EvidenceDocument35 pagesEvidence-Inspired Advocacy and Advocacy-Based EvidencePresentaciones_FKNo ratings yet
- Closing The Cancer DivideDocument36 pagesClosing The Cancer DividePresentaciones_FKNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Health System Responses To Women's Cancers in The AmericasDocument36 pagesHealth System Responses To Women's Cancers in The AmericasPresentaciones_FKNo ratings yet
- Closing The Cancer Divide: Lessons From Women's HealthDocument43 pagesClosing The Cancer Divide: Lessons From Women's HealthPresentaciones_FKNo ratings yet
- Closing The Cancer Divide For Women in The Americas: Diagonal Health System InnovationsDocument39 pagesClosing The Cancer Divide For Women in The Americas: Diagonal Health System InnovationsPresentaciones_FKNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Evidence-Inspired Advocacy and Advocacy-Based EvidenceDocument35 pagesEvidence-Inspired Advocacy and Advocacy-Based EvidencePresentaciones_FKNo ratings yet
- Women's Cancers in The Americas: Closing DividesDocument35 pagesWomen's Cancers in The Americas: Closing DividesPresentaciones_FKNo ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument16 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument18 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- Closing The Cancer Divide: Challenges and OpportunitiesDocument51 pagesClosing The Cancer Divide: Challenges and OpportunitiesPresentaciones_FKNo ratings yet
- Closing Divides To Meet The Challenge of Women S CancerDocument22 pagesClosing Divides To Meet The Challenge of Women S CancerPresentaciones_FKNo ratings yet
- Reducing The Cancer Divide For Breast and Cervical CancerDocument53 pagesReducing The Cancer Divide For Breast and Cervical CancerPresentaciones_FKNo ratings yet
- Women's Cancer Transition: Challenge For Global Health and Health SystemsDocument58 pagesWomen's Cancer Transition: Challenge For Global Health and Health SystemsPresentaciones_FKNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
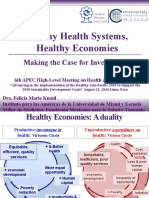
- Healthy Health Systems, Healthy Economies. Making The Case For Investment.Document28 pagesHealthy Health Systems, Healthy Economies. Making The Case For Investment.Presentaciones_FKNo ratings yet
- NCP Deficient Fluid VolumeDocument5 pagesNCP Deficient Fluid VolumeCHRISTINE GRACE ELLONo ratings yet
- Alphaland's Malaria Profile and Control EffortsDocument18 pagesAlphaland's Malaria Profile and Control EffortsAndres RomeroNo ratings yet
- Therapeutics Materia Medica and The Practice of Medicine 1905Document330 pagesTherapeutics Materia Medica and The Practice of Medicine 1905A. K. MohiuddinNo ratings yet
- The SEX COLLECTORS - Vol 1 - 40 Page Sample For Web - 11 March 2010Document40 pagesThe SEX COLLECTORS - Vol 1 - 40 Page Sample For Web - 11 March 2010Cristina Lemoing100% (1)
- Care of The Patient After ThoracotomyDocument12 pagesCare of The Patient After ThoracotomyRaymond EdgeNo ratings yet
- 6 Signs Your Body Is Screaming For HealthDocument44 pages6 Signs Your Body Is Screaming For HealthBlasterWorm100% (1)
- 2016 January FebruaryDocument45 pages2016 January FebruaryAndriusjo100% (1)
- r2017 Open Elective Ece - by Learnengineering - inDocument58 pagesr2017 Open Elective Ece - by Learnengineering - insivakumar0% (1)
- BookletDocument26 pagesBookletapi-261829418No ratings yet
- Brochure For ThalassemiaDocument2 pagesBrochure For ThalassemiaaderindNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ayurvedic Treatment of Enlarged Prostate GlandDocument28 pagesAyurvedic Treatment of Enlarged Prostate GlandRajeshKizziNo ratings yet
- Survey Questionnaire FinalDocument2 pagesSurvey Questionnaire FinalJosie MercyNo ratings yet
- Literature ReviewDocument38 pagesLiterature ReviewAkash PagareNo ratings yet
- Edited Psyche DrugsDocument49 pagesEdited Psyche Drugsa_lavina02No ratings yet
- Discharge Planning and NCP SDocument8 pagesDischarge Planning and NCP SRainier RamosNo ratings yet
- Winshock PDF - GBDocument6 pagesWinshock PDF - GBchamsedineNo ratings yet
- Leo Atp IvDocument25 pagesLeo Atp IvLeonardo MedinaNo ratings yet
- Dermatoses of PregnancyDocument68 pagesDermatoses of PregnancypksaraoNo ratings yet
- Indian Childhood CirrhosisDocument10 pagesIndian Childhood CirrhosisMona Morris89% (9)
- Nasopharyngeal Angiofibroma Treatment OptionsDocument51 pagesNasopharyngeal Angiofibroma Treatment OptionsAbhishek ShahNo ratings yet
- Benefits of Spa Treatments For Mental and Body HealthDocument3 pagesBenefits of Spa Treatments For Mental and Body HealthsuryaningNo ratings yet
- Guidelines For PMDT in India - May 2012Document199 pagesGuidelines For PMDT in India - May 2012smbawasainiNo ratings yet
- Addiction and Self-Control - Perspectives From Philosophy, Psychology, and Neuroscience (2013) PDFDocument289 pagesAddiction and Self-Control - Perspectives From Philosophy, Psychology, and Neuroscience (2013) PDFLouiNo ratings yet
- A Brief Overview of Insomnia by DR Gordon CoatesDocument17 pagesA Brief Overview of Insomnia by DR Gordon CoatesgordoncoatesNo ratings yet
- Clarinase Repetabs Leaflet (Eng) - CCDS 122013-2014-06-26Document2 pagesClarinase Repetabs Leaflet (Eng) - CCDS 122013-2014-06-26Andrew LienataNo ratings yet
- Newsletter - Rob S Vol 4 April 2015Document7 pagesNewsletter - Rob S Vol 4 April 2015api-323491985No ratings yet
- Sexual terms dictionaryDocument3 pagesSexual terms dictionaryGabriela L MarinNo ratings yet
- Bosniak ClassificationDocument19 pagesBosniak ClassificationGirish Kumar100% (1)
- Triage and Disaster ManagementDocument19 pagesTriage and Disaster ManagementCodillia CheongNo ratings yet
- Dengue Discharge PlanDocument1 pageDengue Discharge PlanChris Denver BancaleNo ratings yet