You might also like
- Atrial Fibrillation HandoutDocument5 pagesAtrial Fibrillation HandoutAlfa AlfinNo ratings yet
- Cardiac Arrest, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCardiac Arrest, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Atrial FibrillationDocument35 pagesAtrial FibrillationKABERA RENE100% (2)
- Post Op CardiacDocument7 pagesPost Op CardiacsimplyputmonicNo ratings yet
- Chest Tube ManagementDocument27 pagesChest Tube ManagementIanne Merh100% (2)
- Acute Coronary SyndromeDocument21 pagesAcute Coronary SyndromeNabil Mosharraf Hossain100% (2)
- Introduction To ECG For NursingDocument75 pagesIntroduction To ECG For NursingRashid AlHamdan100% (1)
- Cardiac AsthmaDocument12 pagesCardiac AsthmaNeupane KsabNo ratings yet
- ECG InterpretationDocument48 pagesECG InterpretationKervayse St.ClairNo ratings yet
- Case Analysis:: Myocardial InfarctionDocument76 pagesCase Analysis:: Myocardial InfarctionIpeNo ratings yet
- Cardiogenic Shock PDFDocument14 pagesCardiogenic Shock PDFAdreiTheTripleANo ratings yet
- Differential Diagnosis of Valvular Heart DiseaseDocument10 pagesDifferential Diagnosis of Valvular Heart DiseaseAbhisek ChatterjeeNo ratings yet
- Managing Mechanical VentilationDocument7 pagesManaging Mechanical VentilationArden QuiambaoNo ratings yet
- Pulmonary Edema: (Acute Heart Failure)Document7 pagesPulmonary Edema: (Acute Heart Failure)james garcia100% (5)
- Assessment of Right Ventricular FunctionDocument41 pagesAssessment of Right Ventricular FunctionAditya MadhavpeddiNo ratings yet
- Congestive Heart FailureDocument17 pagesCongestive Heart FailureLyana StarkNo ratings yet
- Status AsthmaticusDocument29 pagesStatus AsthmaticusDavid OlsonNo ratings yet
- Transposition of The Great ArteriesDocument17 pagesTransposition of The Great ArteriesGaram Esther GohNo ratings yet
- Tension Pneumothorax 170102133730Document21 pagesTension Pneumothorax 170102133730novelraaaNo ratings yet
- PneumothoraxDocument52 pagesPneumothoraxtrisna satrianaNo ratings yet
- Cardiac TamponadeDocument10 pagesCardiac TamponadeRahmi Fatma SariNo ratings yet
- Post Resus CareDocument35 pagesPost Resus Caredrjaikrish100% (1)
- Emergency Drugs KathDocument29 pagesEmergency Drugs Kathmajin655No ratings yet
- Intra Aortic Balloon PumpDocument5 pagesIntra Aortic Balloon PumpZainal 'babeh' Arifin100% (1)
- Arterial LinesDocument13 pagesArterial LinesYee LengNo ratings yet
- Acuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiesDocument16 pagesAcuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiessamuelNo ratings yet
- Case Study AllDocument22 pagesCase Study AllGeraldine Gallaron - CasipongNo ratings yet
- Pulmonary EmbolismDocument80 pagesPulmonary EmbolismVarun B Renukappa100% (1)
- Valvular Heart DiseaseDocument2 pagesValvular Heart DiseaseAnonymous TVk12eX4No ratings yet
- Cardiac CatheterizationDocument2 pagesCardiac Catheterizationjacallis50% (2)
- Critical Care/Intensive Care Unit Experience Internal Medicine INM.M INM.S CourseDocument11 pagesCritical Care/Intensive Care Unit Experience Internal Medicine INM.M INM.S CourseAmer Moh SarayrahNo ratings yet
- Abcde ApproachDocument3 pagesAbcde ApproachMaria Isabel Medina MesaNo ratings yet
- Ecg 01Document103 pagesEcg 01Bandar al ghamdi100% (1)
- 1st, 2nd, 3rd Degree AV BLockDocument8 pages1st, 2nd, 3rd Degree AV BLockladydreamer_92No ratings yet
- Possible Cardiac Chest Pain Clinical Pathway: FacilityDocument2 pagesPossible Cardiac Chest Pain Clinical Pathway: FacilityshofiyuddinNo ratings yet
- Atrial Fibrillation CASE STUDYDocument2 pagesAtrial Fibrillation CASE STUDYChristianneMikeNo ratings yet
- Nursing Management: Nursing Management: Acute Kidney Injury and Chronic Kidney DiseaseDocument22 pagesNursing Management: Nursing Management: Acute Kidney Injury and Chronic Kidney Diseasedian rachmat saputroNo ratings yet
- Hypoglycemia: Presented by Farse GhabayenDocument11 pagesHypoglycemia: Presented by Farse GhabayenFares G. Ghabayen100% (2)
- Inotropes, Excellent Article, With DosingDocument47 pagesInotropes, Excellent Article, With DosingNavojit ChowdhuryNo ratings yet
- ECG StudyDocument32 pagesECG StudyDan Daniel XuNo ratings yet
- Cardio Lab MedsDocument11 pagesCardio Lab MedsDianne Erika MeguinesNo ratings yet
- Hypertensive CrisisDocument28 pagesHypertensive CrisisJacob Alexander MarpaungNo ratings yet
- Arrhythmia Diagnosis and ManagementDocument44 pagesArrhythmia Diagnosis and ManagementanwarNo ratings yet
- Blood Transfusion ESSAY 1 1Document3 pagesBlood Transfusion ESSAY 1 1Ednilson Domingos0% (1)
- Renal Failure PresentationDocument65 pagesRenal Failure PresentationBhawna JoshiNo ratings yet
- Kuliah Ekg UnswagatiDocument75 pagesKuliah Ekg UnswagatiiikNo ratings yet
- Vasopressor & InotropesDocument44 pagesVasopressor & InotropesArun KumarNo ratings yet
- Infective Diseases of Heart: Wella KarolinaDocument47 pagesInfective Diseases of Heart: Wella KarolinahayosiapaNo ratings yet
- Anticoagulation in Hemodialysis: Arlene S. Munoz MD, FPCP, FPSNDocument51 pagesAnticoagulation in Hemodialysis: Arlene S. Munoz MD, FPCP, FPSNBryant MunozNo ratings yet
- Cardiogenic ShockDocument5 pagesCardiogenic ShockAttilio Del RossoNo ratings yet
- Peritonitis in PD PatientsDocument64 pagesPeritonitis in PD PatientsDaniel SitungkirNo ratings yet
- Ecg 1Document40 pagesEcg 1doctorhanifNo ratings yet
- Acute Rheumatic FeverDocument50 pagesAcute Rheumatic Feversunaryo lNo ratings yet
- Aclsrhythmtest11 PDFDocument7 pagesAclsrhythmtest11 PDFmonir610% (1)
- Acute Respiratory Distress SyndromeDocument70 pagesAcute Respiratory Distress SyndromeAndrea Del Villar100% (1)
- Congestive Heart FailureDocument43 pagesCongestive Heart FailuresudersonNo ratings yet
- Arterial Line and Central LineDocument32 pagesArterial Line and Central LineOrachorn AimarreeratNo ratings yet
- Food ContaminationDocument19 pagesFood Contaminationfarmasi_hm100% (2)
- Management of Septic Shock in AdultsDocument28 pagesManagement of Septic Shock in Adultsfarmasi_hmNo ratings yet
- Major Depressive DisordersDocument22 pagesMajor Depressive Disordersfarmasi_hm100% (2)
- Glargine and CancerDocument13 pagesGlargine and Cancerfarmasi_hmNo ratings yet
- Emergency ContraceptionDocument24 pagesEmergency Contraceptionfarmasi_hm100% (1)
- Head LiceDocument15 pagesHead Licefarmasi_hmNo ratings yet
- Peptic Ulcer DiseaseDocument26 pagesPeptic Ulcer Diseasefarmasi_hmNo ratings yet
- AcneDocument24 pagesAcnefarmasi_hm100% (2)
- New & Emerging Treatment of Diabetic Retinopathy: Presented By: Pauline Teo Siew Chin 7th January, 2009Document42 pagesNew & Emerging Treatment of Diabetic Retinopathy: Presented By: Pauline Teo Siew Chin 7th January, 2009farmasi_hmNo ratings yet
- Presented By: Siti Noraisah BT KifliDocument28 pagesPresented By: Siti Noraisah BT Kiflifarmasi_hmNo ratings yet
- Diabetic KetoacidosisDocument12 pagesDiabetic Ketoacidosisfarmasi_hmNo ratings yet
- WarfarinDocument21 pagesWarfarinfarmasi_hmNo ratings yet
- Syndrome of Inappropriate Secretion of Anti Diuretic HormoneDocument39 pagesSyndrome of Inappropriate Secretion of Anti Diuretic Hormonefarmasi_hmNo ratings yet
- Medication Safety UnitDocument58 pagesMedication Safety Unitfarmasi_hmNo ratings yet
- ADR Reporting, Medication Error Reporting SystemDocument100 pagesADR Reporting, Medication Error Reporting Systemfarmasi_hm100% (1)
- Deep Vein Thrombosis - 2003Document34 pagesDeep Vein Thrombosis - 2003farmasi_hm100% (1)
- Atopic Dermatitis (Eczema)Document19 pagesAtopic Dermatitis (Eczema)farmasi_hmNo ratings yet
- Sinusitis & Its TreatmentDocument20 pagesSinusitis & Its Treatmentfarmasi_hmNo ratings yet
- Diuretics: Sumolly Anak DavidDocument29 pagesDiuretics: Sumolly Anak Davidfarmasi_hmNo ratings yet
- HPV Infection StephDocument25 pagesHPV Infection Stephfarmasi_hmNo ratings yet
- Leptospirosis: Pauline Teo Siew ChinDocument18 pagesLeptospirosis: Pauline Teo Siew Chinfarmasi_hmNo ratings yet
- Angiotensin Receptor Blockers (O)Document26 pagesAngiotensin Receptor Blockers (O)farmasi_hmNo ratings yet
- Otc Treatment For Muscle Sprain & StrainsDocument12 pagesOtc Treatment For Muscle Sprain & Strainsfarmasi_hmNo ratings yet
- Overview of Nephrotic SyndromeDocument19 pagesOverview of Nephrotic Syndromefarmasi_hm100% (1)
- IntroductionDocument21 pagesIntroductionfarmasi_hmNo ratings yet
- Hyperemesis GravidarumDocument13 pagesHyperemesis GravidarumBang JuntakNo ratings yet
- OTC PregnancyDocument11 pagesOTC Pregnancyfarmasi_hmNo ratings yet
- Calcium Channel BlockersDocument15 pagesCalcium Channel Blockersfarmasi_hm100% (2)
- Over-The-Counter Foot CareDocument17 pagesOver-The-Counter Foot Carefarmasi_hmNo ratings yet
- Supraventricular Tachycardia: Birmingham Children's Hospital ED Handbook Version 1 (2011)Document1 pageSupraventricular Tachycardia: Birmingham Children's Hospital ED Handbook Version 1 (2011)madimadi11No ratings yet
- Ghid de Resuscitare Dupa Chirurgia Cardiaca EACTS 2009Document24 pagesGhid de Resuscitare Dupa Chirurgia Cardiaca EACTS 2009Raluca L100% (1)
- Amiodarone IV Administration 1.0Document5 pagesAmiodarone IV Administration 1.0Ari BinkosimNo ratings yet
- Supra Ventricular TachycardiaDocument10 pagesSupra Ventricular TachycardiaJohn RobinsonNo ratings yet
- Amiodarone (PACERONE)Document1 pageAmiodarone (PACERONE)Amanda CoadNo ratings yet
- Emergency Parenteral Drugs ListDocument4 pagesEmergency Parenteral Drugs ListRem Remoreras75% (4)
- ACLS DrugDocument7 pagesACLS DrugPhongsatorn Thunin100% (1)
- Pharmacology Misbah PDFDocument238 pagesPharmacology Misbah PDFRiham Khamis86% (7)
- (See Details in DRUGDEX®) : Adult DosingDocument13 pages(See Details in DRUGDEX®) : Adult Dosingkinko6No ratings yet
- All Uworld Notes 2019 Nclex Nursing ResourcesDocument152 pagesAll Uworld Notes 2019 Nclex Nursing Resourcesnene lewis100% (1)
- Paramedic Drugs in EMSDocument12 pagesParamedic Drugs in EMSJim Hoffman100% (4)
- Atrial FibrillationDocument55 pagesAtrial FibrillationNikhil Kumar100% (1)
- Antiaritmia: Frans D. Suyatna Modified by Sulistia 1010 Departemen Farmakologi & Terapeutik FKUIDocument56 pagesAntiaritmia: Frans D. Suyatna Modified by Sulistia 1010 Departemen Farmakologi & Terapeutik FKUIJoshua ObrienNo ratings yet
- Drug Main ACLS Use Dose/Route NotesDocument4 pagesDrug Main ACLS Use Dose/Route NotesshadyNo ratings yet
- Chapter 5 Drug StudyDocument16 pagesChapter 5 Drug StudyRegee Rose LacsonNo ratings yet
- Cardiovascular Pharmacology: DR Muhamad Ali Sheikh Abdul Kader MD (Usm) MRCP (Uk) Cardiologist, Penang HospitalDocument63 pagesCardiovascular Pharmacology: DR Muhamad Ali Sheikh Abdul Kader MD (Usm) MRCP (Uk) Cardiologist, Penang HospitalCvt RasulNo ratings yet
- Basaria 2005 DDDocument9 pagesBasaria 2005 DDCosmin GabrielNo ratings yet
- Aha Acls Prep Packet 2021 NewDocument69 pagesAha Acls Prep Packet 2021 Newdim100% (2)
- Complete Drug StudyDocument239 pagesComplete Drug StudyRPh Krishna Chandra Jagrit0% (1)
- Drug Induced Optic NeuropathyDocument23 pagesDrug Induced Optic NeuropathyFaizi JaniNo ratings yet
- Drug Interaction MonitoringDocument5 pagesDrug Interaction MonitoringAnonymousNo ratings yet
- Emergency DrugsDocument7 pagesEmergency DrugsMarie Angeline ManzanoNo ratings yet
- Arritmias VentricularesDocument11 pagesArritmias VentricularesJesusIsmaelCoronaNo ratings yet
- Pharm Exam1Document17 pagesPharm Exam1Jill Putman Beistline75% (4)
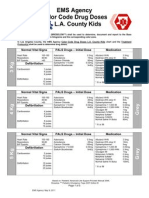
- EMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationDocument5 pagesEMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationCruz VerdeNo ratings yet
- Ecart MedicationsDocument39 pagesEcart Medicationsanon_140774008No ratings yet
- Amiodarone by AymanDocument37 pagesAmiodarone by AymanSabrina ShalhoutNo ratings yet
- ACLS PharmacologyDocument5 pagesACLS PharmacologyKim Still ChunnNo ratings yet
- Antimicrobial Drug Interactionstable220716 PDFDocument4 pagesAntimicrobial Drug Interactionstable220716 PDFBhavin DesaiNo ratings yet
- PVC Unido ConDuplicadosDocument1,181 pagesPVC Unido ConDuplicadosJorge Chachaima MarNo ratings yet