You might also like
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pathophysiology of HyperthyroidismDocument4 pagesPathophysiology of HyperthyroidismKitty YuffieNo ratings yet
- CholelithiasisDocument6 pagesCholelithiasismarkzamNo ratings yet
- CHF Group 3 Ncmb312 RleDocument39 pagesCHF Group 3 Ncmb312 RleMaica Lectana50% (2)
- Pathophysiology of Urinary Tract ObstructionDocument50 pagesPathophysiology of Urinary Tract ObstructionPryo UtamaNo ratings yet
- Case 1 - Pneumonia (Final)Document4 pagesCase 1 - Pneumonia (Final)Joegie ArioNo ratings yet
- Acute BronchitisDocument38 pagesAcute BronchitisNikko MelencionNo ratings yet
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocument43 pagesPamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaNo ratings yet
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 pagesDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいNo ratings yet
- Schematic Diagram Pathophysiology (Book-Based) COPD and TuberculosisDocument1 pageSchematic Diagram Pathophysiology (Book-Based) COPD and Tuberculosispragna novaNo ratings yet
- Hypertension Pathophysiology and Treatment PDFDocument6 pagesHypertension Pathophysiology and Treatment PDFBella TogasNo ratings yet
- Anatomy and Phsyiology of MeningococcemiaDocument2 pagesAnatomy and Phsyiology of MeningococcemiaKevin Comahig100% (1)
- Pleural EffusionDocument3 pagesPleural EffusionEjie Boy IsagaNo ratings yet
- Tuberculous MeningitisDocument11 pagesTuberculous MeningitiszuhriNo ratings yet
- USC Case 04 - SinusitisDocument9 pagesUSC Case 04 - SinusitisDisti Damelia SebayangNo ratings yet
- DimenhydrinateDocument2 pagesDimenhydrinateNinoska Garcia-Ortiz100% (1)
- Pneumonia PathoDocument2 pagesPneumonia PathoDerick Nyl PascualNo ratings yet
- Insulin EffectsDocument24 pagesInsulin Effectsvag taoNo ratings yet
- NCP-Case Presentation (CHF)Document4 pagesNCP-Case Presentation (CHF)Jessamine EnriquezNo ratings yet
- NCP CvaDocument4 pagesNCP CvaMariquita BuenafeNo ratings yet
- Cor-Pulmonale PathophysiologyDocument1 pageCor-Pulmonale PathophysiologyAlyssa Mae Radam100% (1)
- BPHDocument81 pagesBPHFlo Neri BerondoNo ratings yet
- Case Study ReportDocument23 pagesCase Study Reportapi-290866384No ratings yet
- Case PresentationDocument6 pagesCase PresentationYrrem UbaganNo ratings yet
- Occurs Most Often In:: Muscular DystrophyDocument4 pagesOccurs Most Often In:: Muscular DystrophyJiezl Abellano AfinidadNo ratings yet
- Oks Na To Thank U Aubs!!: Okiii!!! Wuv U All!Document10 pagesOks Na To Thank U Aubs!!: Okiii!!! Wuv U All!CiaraNo ratings yet
- Post Cesarean Section DeliveryDocument5 pagesPost Cesarean Section Deliveryᒙᕧᖇᕦᙏᖻ ᗴᔛᓦᗩᖆᗩNo ratings yet
- Mesna: Mesna, Sold Under The BrandDocument17 pagesMesna: Mesna, Sold Under The BrandAndry HamdaniNo ratings yet
- Influenza PATHOPHYSIOLOGYDocument3 pagesInfluenza PATHOPHYSIOLOGYElle RosalesNo ratings yet
- Concept MapDocument3 pagesConcept MapKevin T. KatadaNo ratings yet
- Addison'sDocument4 pagesAddison'sKoRnflakesNo ratings yet
- ParacetamolDocument2 pagesParacetamolsleep whatNo ratings yet
- Thyroid Papillary Carcinoma CaseDocument6 pagesThyroid Papillary Carcinoma CaseRandy F BabaoNo ratings yet
- Pathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsDocument4 pagesPathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsLovely DaroleNo ratings yet
- NCP - Impaired Gas Exchange (COPD)Document3 pagesNCP - Impaired Gas Exchange (COPD)Karen Joy ItoNo ratings yet
- Capital Budgetting ReportDocument9 pagesCapital Budgetting ReportAhmed HadiNo ratings yet
- Generic Name: Ceftriaxone Brand Name: (Kept Rix) IV, 1g, q12Document5 pagesGeneric Name: Ceftriaxone Brand Name: (Kept Rix) IV, 1g, q12De Sesto Rhys CarloNo ratings yet
- CASE STUDY PheumoniaDocument5 pagesCASE STUDY PheumoniaEdelweiss Marie CayetanoNo ratings yet
- The Patient and His Illness A. Pathophysiology (Book Based)Document5 pagesThe Patient and His Illness A. Pathophysiology (Book Based)Edmar Francis SabileNo ratings yet
- Case Study Ugib Lower MBDocument65 pagesCase Study Ugib Lower MBQuolette Constante100% (1)
- HCVDDocument5 pagesHCVDkhrizaleehNo ratings yet
- NCP Poststreptococcal GlomerulonephritisDocument12 pagesNCP Poststreptococcal GlomerulonephritisScarlet ScarletNo ratings yet
- Diabetes PathoDocument2 pagesDiabetes Pathodrewcel100% (1)
- Risk For Bleeding - Cirrhosis NCPDocument2 pagesRisk For Bleeding - Cirrhosis NCPPaula AbadNo ratings yet
- MedSurg Notes - Cancer of The LiverDocument2 pagesMedSurg Notes - Cancer of The LiverMae CeaesarNo ratings yet
- NCP - Poststreptococcal GlomerulonephritisDocument12 pagesNCP - Poststreptococcal GlomerulonephritisAya BolinasNo ratings yet
- Drug Study - PiptazDocument1 pageDrug Study - PiptazMutya XDNo ratings yet
- Anal Canal: Fissure in Ano HaemorrhoidsDocument37 pagesAnal Canal: Fissure in Ano Haemorrhoidsyash shrivastavaNo ratings yet
- Case Stydy Angina PectorisDocument46 pagesCase Stydy Angina PectorissharenNo ratings yet
- NCPDocument10 pagesNCPRobin HaliliNo ratings yet
- Pathophysiology of Portal HYPERTENSION PDFDocument11 pagesPathophysiology of Portal HYPERTENSION PDFCamilo VidalNo ratings yet
- Case Pres A1-RhdDocument11 pagesCase Pres A1-RhdCharm TanyaNo ratings yet
- Acute Lymphoblastic LeukemiaDocument34 pagesAcute Lymphoblastic LeukemiamtyboyNo ratings yet
- Concept Map 5Document2 pagesConcept Map 5api-354331689No ratings yet
- Anatomy and Physiology of NeonatesDocument17 pagesAnatomy and Physiology of NeonatesYu ShiNo ratings yet
- Case Study 1 (Pneumonia)Document13 pagesCase Study 1 (Pneumonia)Kate EscotonNo ratings yet
- Pleural EffusionDocument51 pagesPleural EffusionMinhajul IslamNo ratings yet
- Pleural Effusion: Dr.S.Sesha Sai (MD), Pulmonary MedicineDocument52 pagesPleural Effusion: Dr.S.Sesha Sai (MD), Pulmonary MedicinevaishnaviNo ratings yet
- Efusi Pleura & EmpyemaDocument47 pagesEfusi Pleura & EmpyemaArumLaksmitaDewiNo ratings yet
- Brochure Health ProfessionsDocument12 pagesBrochure Health ProfessionsWan HafizNo ratings yet
- Nihms 632585jjkjkDocument18 pagesNihms 632585jjkjkWan HafizNo ratings yet
- Market Analysis For Three Peruvian Natural Ingredients For Web PDFDocument160 pagesMarket Analysis For Three Peruvian Natural Ingredients For Web PDFatninirrrNo ratings yet
- With Examples, What Are The Properties of An Ideal Tumour Marker?Document43 pagesWith Examples, What Are The Properties of An Ideal Tumour Marker?Wan HafizNo ratings yet
- Research Nih 3399393Document15 pagesResearch Nih 3399393Wan HafizNo ratings yet
- Faq BiDocument2 pagesFaq BiShuhaidah SalehinNo ratings yet
- CPG Management of Acute ST Elevation Myocardial Infarction (STEMI) (4th Ed) 2019 PDFDocument148 pagesCPG Management of Acute ST Elevation Myocardial Infarction (STEMI) (4th Ed) 2019 PDFTham HahaNo ratings yet
- Homonculus Dot Dot DotDocument10 pagesHomonculus Dot Dot DotWan HafizNo ratings yet
- Hyponatremia (Essay)Document3 pagesHyponatremia (Essay)Wan HafizNo ratings yet
- DIabetes InsipidusDocument3 pagesDIabetes InsipidusWan HafizNo ratings yet
- Ebook Blood Transfusion Guideline PDFDocument170 pagesEbook Blood Transfusion Guideline PDFFazley Izuddin100% (1)
- Atoto CompilationDocument100 pagesAtoto CompilationWan HafizNo ratings yet
- Cushing Syndrome EssayDocument6 pagesCushing Syndrome EssayWan HafizNo ratings yet
- Diabetes Mellitus ComplicationDocument4 pagesDiabetes Mellitus ComplicationWan HafizNo ratings yet
- Efficacy of Fluorochrome Stain in The Diagnosis of Pulmonary Tuberculosis Co-Infected With HIV - B - K Prasanthi, AR Kumari - B - , Indian Journal of Medical Microbiology PDFDocument4 pagesEfficacy of Fluorochrome Stain in The Diagnosis of Pulmonary Tuberculosis Co-Infected With HIV - B - K Prasanthi, AR Kumari - B - , Indian Journal of Medical Microbiology PDFWan HafizNo ratings yet
- TRD 78 47Document9 pagesTRD 78 47adindadian12No ratings yet
- Lecciones Basicas en Control de Calidad.2008 Bio-Rad InglesDocument62 pagesLecciones Basicas en Control de Calidad.2008 Bio-Rad InglesPili Gabriel67% (3)
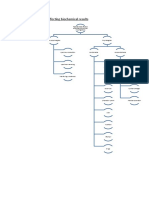
- Preanalytical Factors Affecting Biochemical ResultsDocument7 pagesPreanalytical Factors Affecting Biochemical ResultsWan HafizNo ratings yet
- Lecciones Basicas en Control de Calidad.2008 Bio-Rad InglesDocument62 pagesLecciones Basicas en Control de Calidad.2008 Bio-Rad InglesPili Gabriel67% (3)
- Where Seamless Living Is Abridged: Site Plan Location MapDocument2 pagesWhere Seamless Living Is Abridged: Site Plan Location MapWan HafizNo ratings yet
- Tuberculosis Natural History, Microbiology, and PathogenesisDocument31 pagesTuberculosis Natural History, Microbiology, and PathogenesisWan HafizNo ratings yet
- A Retrospective Analysis of Treatment Outcomes of Drug-Susceptible TB in Kazakhstan, 2013-2016Document14 pagesA Retrospective Analysis of Treatment Outcomes of Drug-Susceptible TB in Kazakhstan, 2013-2016Wan HafizNo ratings yet
- A Modified Acid-Fast Staining Method For Rapid Detection ofDocument5 pagesA Modified Acid-Fast Staining Method For Rapid Detection ofWan HafizNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Pneumonia and Respiratory Tract Infections in ChildrenDocument37 pagesPneumonia and Respiratory Tract Infections in ChildrenjayasiinputNo ratings yet
- No Added Value of Performing Ziehl-Neelsen OnDocument7 pagesNo Added Value of Performing Ziehl-Neelsen OnWan HafizNo ratings yet
- 0730 Cunningham Fluids and Electrolytes 2012Document19 pages0730 Cunningham Fluids and Electrolytes 2012Wan HafizNo ratings yet
- Ligature Material in HangingDocument5 pagesLigature Material in HangingWan HafizNo ratings yet
- 0730 Cunningham Fluids and Electrolytes 2012Document19 pages0730 Cunningham Fluids and Electrolytes 2012Wan HafizNo ratings yet
- Preface: Hematopathology Book, The Editors Decided For A Major ReviDocument1 pagePreface: Hematopathology Book, The Editors Decided For A Major ReviWan HafizNo ratings yet
- Schoolgirl: María de Los Ángeles Lizeth Solís Jiménez Teacher: Kenneth Matter: English VDocument16 pagesSchoolgirl: María de Los Ángeles Lizeth Solís Jiménez Teacher: Kenneth Matter: English VAngeles Solis JimenezNo ratings yet
- Chapter III Pharmacokinetics: Durge Raj GhalanDocument64 pagesChapter III Pharmacokinetics: Durge Raj GhalanDurge Raj Ghalan100% (3)
- 2017 ESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST Segment ElevationDocument66 pages2017 ESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST Segment ElevationMoises Torres AlvarezNo ratings yet
- Cookery 1 Module 4 g11Document12 pagesCookery 1 Module 4 g11Rochel SistonaNo ratings yet
- Alexander 2023 My Left KidneyDocument87 pagesAlexander 2023 My Left KidneyStamnumNo ratings yet
- Brubaker 2001Document5 pagesBrubaker 2001Residencia OftalmologíaNo ratings yet
- Pilferage Control in HospitalsDocument4 pagesPilferage Control in HospitalsDr. Rakshit Solanki100% (3)
- Indaegu: Exclusive Interview With Usain Bolt and His Agent, Ricky SimmsDocument13 pagesIndaegu: Exclusive Interview With Usain Bolt and His Agent, Ricky SimmsCraig WhiteNo ratings yet
- Giant Cell Tumor of Bone - An Overview: Current Concepts ReviewDocument8 pagesGiant Cell Tumor of Bone - An Overview: Current Concepts ReviewDwi fitria nivaNo ratings yet
- Reflective Journal 1 2 and 3Document11 pagesReflective Journal 1 2 and 3api-321980896No ratings yet
- Headache Management Guideline For Adults Version 10Document6 pagesHeadache Management Guideline For Adults Version 10TomiNo ratings yet
- K3 Bidang Pertanian ILO PDFDocument350 pagesK3 Bidang Pertanian ILO PDFSufyan StauriNo ratings yet
- 3GN18CV402 Internship ReportDocument29 pages3GN18CV402 Internship ReportHP PAVILION100% (1)
- Reflection PaperDocument27 pagesReflection PaperBon Ryan LeonardoNo ratings yet
- User's Manual: M200A Syringe PumpDocument44 pagesUser's Manual: M200A Syringe PumpGandavaa Enkhee50% (4)
- Patient Monitor PC-5000 User Manual PDFDocument85 pagesPatient Monitor PC-5000 User Manual PDFdanniel9090100% (1)
- ChlamydiaDocument3 pagesChlamydiaapi-280196750No ratings yet
- C0mponents of A Logic ModelDocument2 pagesC0mponents of A Logic Modelsameer mohamudallyNo ratings yet
- Minimum and Peak Flows of WastewaterDocument26 pagesMinimum and Peak Flows of WastewaterSteven Joseph IncioNo ratings yet
- POCSODocument15 pagesPOCSOThakur Avnish Singh100% (1)
- PD 1067 Water Code of The Philippines and Clean Water ActDocument44 pagesPD 1067 Water Code of The Philippines and Clean Water ActNovy Jamboy Ragmac100% (2)
- Daftar PustakaDocument3 pagesDaftar PustakaTeguh firmansyahNo ratings yet
- 2020 Status Report As of August 31, 2021Document192 pages2020 Status Report As of August 31, 2021Jasper Kenneth PeraltaNo ratings yet
- Biphasic and Polyphasic SleepDocument6 pagesBiphasic and Polyphasic SleepalNo ratings yet
- Family Reunification Plan Template FINAL 8-31-17 Incl. Appendices Pages All PortraitDocument146 pagesFamily Reunification Plan Template FINAL 8-31-17 Incl. Appendices Pages All PortraitLloyd Angelo SobredillaNo ratings yet
- Arena - Experimental Homeopathic Research On Opuntia Ficus IndicaDocument8 pagesArena - Experimental Homeopathic Research On Opuntia Ficus IndicaAnny Kelly VasconcelosNo ratings yet
- Agama Dan Spiritualitas Dalam Konteks Kesehatan Dan KeperawatanDocument28 pagesAgama Dan Spiritualitas Dalam Konteks Kesehatan Dan KeperawatanSELVI AQILAHNo ratings yet
- 2021 A Guide To The African Human Rights System Celebrating 40 YearsDocument115 pages2021 A Guide To The African Human Rights System Celebrating 40 YearsChala Yuye KemerNo ratings yet
- Review Jurnal Varicella - Dewi Manik Aulia Fadli - 16700096Document26 pagesReview Jurnal Varicella - Dewi Manik Aulia Fadli - 16700096Lia FadliNo ratings yet
- Logic ModelDocument2 pagesLogic ModelstojannaNo ratings yet