You might also like
- Care Under Fire: Tactical Combat Casualty Care For Medical Personnel August 2018Document84 pagesCare Under Fire: Tactical Combat Casualty Care For Medical Personnel August 2018alyssaNo ratings yet
- TCCC CourseDocument22 pagesTCCC CourseSteve Fetalino Demaala100% (1)
- Tactical Casualty Combat Care Handbook v5 PDFDocument133 pagesTactical Casualty Combat Care Handbook v5 PDFJose Torres100% (5)
- How To Become A Successful Bodyguard: Alternative Careers Series, #6From EverandHow To Become A Successful Bodyguard: Alternative Careers Series, #6No ratings yet
- USArmy SOF CasualtyCareDocument66 pagesUSArmy SOF CasualtyCarepisnyri100% (5)
- Warm Zone Active ShooterDocument13 pagesWarm Zone Active ShooterKarl Kiw-isNo ratings yet
- Intro To Tactical MedicineDocument70 pagesIntro To Tactical MedicinePaula Pinto Beerens100% (4)
- Chapter 1 Tactical Combat Casualty CareDocument52 pagesChapter 1 Tactical Combat Casualty Care120v60hz100% (1)
- 01 Intro To TCCC For All Combatants 140602Document53 pages01 Intro To TCCC For All Combatants 140602Bruno100% (1)
- 0779 NATO SOF Medical Standards and Training 2009Document78 pages0779 NATO SOF Medical Standards and Training 2009freemedicNo ratings yet
- Tactical Combat Casualty CareDocument88 pagesTactical Combat Casualty CareFirefighther Ayala100% (4)
- TCCCDocument117 pagesTCCCthallesnet100% (3)
- TCCC Special OperationsDocument15 pagesTCCC Special OperationsPablo Guiote100% (1)
- Survival First Aid: How to treat injuries and save livesFrom EverandSurvival First Aid: How to treat injuries and save livesRating: 5 out of 5 stars5/5 (1)
- Personal Security Detail Operations Book 2: Personal Security Detail Operations, #2From EverandPersonal Security Detail Operations Book 2: Personal Security Detail Operations, #2No ratings yet
- Call of Duty Division: MOUT TacticsDocument9 pagesCall of Duty Division: MOUT Tacticssimenbrunstad100% (1)
- Surviving Vehicle AmbushDocument3 pagesSurviving Vehicle AmbushAaron CunninghamNo ratings yet
- Special Operations ForcesDocument108 pagesSpecial Operations Forcessaz08100% (1)
- RDPR Lesson Plan - Ialefi 2012 AtcDocument60 pagesRDPR Lesson Plan - Ialefi 2012 AtclucamorlandoNo ratings yet
- TacticalMedicineManual July6Document78 pagesTacticalMedicineManual July6Flighterdoc100% (10)
- Close Quarters Combat CQCDocument28 pagesClose Quarters Combat CQCMarcos Daniel Schmidt GarofaloNo ratings yet
- 1 Introduction To TCCC USA 20015Document47 pages1 Introduction To TCCC USA 20015Jorge Almeida CostaNo ratings yet
- Call TCCC Handbook 1203Document86 pagesCall TCCC Handbook 1203Esteban Carrero100% (1)
- TCCC Guidelines 15th Dec 2021Document19 pagesTCCC Guidelines 15th Dec 2021Arturo100% (1)
- Tactical Emergency Casualty Care Field GuideFrom EverandTactical Emergency Casualty Care Field GuideRating: 3 out of 5 stars3/5 (1)
- Tactical Combat Casualty CareDocument114 pagesTactical Combat Casualty Caresrtmedic100% (5)
- Active Shooter TrainingDocument33 pagesActive Shooter Trainingapi-298765135No ratings yet
- Close Quarters Marksmanship/Battle (CQM/CQB) : August 2006Document27 pagesClose Quarters Marksmanship/Battle (CQM/CQB) : August 2006Jefferson SanchezNo ratings yet
- How to Survive a Terrorist Attack – Become Prepared for a Bomb Threat or Active Shooter Assault: Save Yourself and the Lives of Others - Learn How to Act Instantly, The Strategies and Procedures After the Incident, How to Help the Injured & Be Able to Provide First AidFrom EverandHow to Survive a Terrorist Attack – Become Prepared for a Bomb Threat or Active Shooter Assault: Save Yourself and the Lives of Others - Learn How to Act Instantly, The Strategies and Procedures After the Incident, How to Help the Injured & Be Able to Provide First AidNo ratings yet
- TECC GuidelinesDocument11 pagesTECC Guidelineserdoc1491No ratings yet
- From Alpha To Omega. A Milsim Tactical Primer and Training ManualDocument206 pagesFrom Alpha To Omega. A Milsim Tactical Primer and Training ManualДмитрий ОрловNo ratings yet
- 1 - Special Operations Combat MedicDocument2 pages1 - Special Operations Combat MedicNeil McCauleyNo ratings yet
- CAT Tourniquet Application GuideDocument2 pagesCAT Tourniquet Application GuidekevinNo ratings yet
- Executive ProtectionDocument3 pagesExecutive Protectionapi-77207723No ratings yet
- Sniper S.O.PDocument38 pagesSniper S.O.PAnonymous KILBAQZNo ratings yet
- DHS Tactical EMS Guide PDFDocument204 pagesDHS Tactical EMS Guide PDFxose lois Lopez100% (2)
- Tactical Combat Casualty Care 1Document132 pagesTactical Combat Casualty Care 1Andre Aguiar100% (1)
- Active Shooter How To RespondDocument13 pagesActive Shooter How To RespondgabrielMeuNomeAquiNo ratings yet
- Active Shooter AzaleaDocument27 pagesActive Shooter AzaleaRJay JacabanNo ratings yet
- TCCC PDFDocument86 pagesTCCC PDFJaime Acevedo100% (1)
- Infantryman 11B Professional Development Model: Rank PVT-PFC SPC-CPL SGT SSG SFC Critical Operational PositionsDocument1 pageInfantryman 11B Professional Development Model: Rank PVT-PFC SPC-CPL SGT SSG SFC Critical Operational Positionsfoxbat05No ratings yet
- Force Protection - IEDs Article03022004bDocument26 pagesForce Protection - IEDs Article03022004bwarrior_2008100% (1)
- Swat Version 2011Document20 pagesSwat Version 2011stjohn45No ratings yet
- SRC PolicialDocument18 pagesSRC PolicialSRC MOZAMBIQUENo ratings yet
- 1 Pararescue Medication and Procedure Handbook 137pagesDocument137 pages1 Pararescue Medication and Procedure Handbook 137pagesFabian LeclercqNo ratings yet
- Active ShooterDocument28 pagesActive Shootercomputerfundi100% (1)
- Atirc PDFDocument378 pagesAtirc PDFTeobaldo Padilla Apari100% (1)
- Ranger Medic Handbook 2007Document154 pagesRanger Medic Handbook 2007Jared A. Lang93% (15)
- Anatomy of A Hostage Rescue - ADA427693Document209 pagesAnatomy of A Hostage Rescue - ADA427693cliftoncage100% (1)
- Active Threat Response Trainings FinalDocument7 pagesActive Threat Response Trainings FinalShawn DownloaderNo ratings yet
- Close Protection - Luxury & Host - Orlando WilsonDocument202 pagesClose Protection - Luxury & Host - Orlando WilsonIan BecksNo ratings yet
- Tactical ProgressionDocument55 pagesTactical ProgressionSiu HeiNo ratings yet
- Pararescue Medication and Procedure Handbook-1Document137 pagesPararescue Medication and Procedure Handbook-1Charles Harris100% (1)
- CrimDocument1 pageCrimEdwin VillaNo ratings yet
- Hubbard Co Jail PlanningDocument8 pagesHubbard Co Jail PlanningShannon GeisenNo ratings yet
- Save Dimmeys. VCAT ORDER. 5 August 2011Document4 pagesSave Dimmeys. VCAT ORDER. 5 August 2011Save Dimmeys100% (1)
- Defaulter Web List BBBDocument20 pagesDefaulter Web List BBBBB ENTERPRISESNo ratings yet
- 3.07.2.13-2.2b Levitsky&Way 2003Document68 pages3.07.2.13-2.2b Levitsky&Way 2003Leandro Hosbalikciyan Di LevaNo ratings yet
- Notice of Dispute - Proof of Claim - Debt Validation Template 8-10-10 Copy 3Document4 pagesNotice of Dispute - Proof of Claim - Debt Validation Template 8-10-10 Copy 3Nessie Jenkins95% (43)
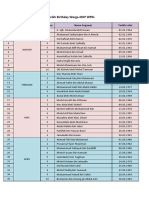
- Tarikh Besday 2023Document4 pagesTarikh Besday 2023Wan Firdaus Wan IdrisNo ratings yet
- Article 7 Sec 4 Legarda V de CastroDocument2 pagesArticle 7 Sec 4 Legarda V de CastroJc Araojo100% (1)
- Dee Chua & Sons v. CIR, G.R. No. L-2216, 31 Jan 1950Document4 pagesDee Chua & Sons v. CIR, G.R. No. L-2216, 31 Jan 1950Ron AceroNo ratings yet
- Tamil Nadu Government Gazette: ExtraordinaryDocument2 pagesTamil Nadu Government Gazette: ExtraordinaryAnushya RamakrishnaNo ratings yet
- Da Pam 600-3-31 Branch Code 31 Military PoliceDocument18 pagesDa Pam 600-3-31 Branch Code 31 Military PoliceMark CheneyNo ratings yet
- Eu EnlargementDocument62 pagesEu EnlargementNeculai CatanaNo ratings yet
- Body Language: While You Are Talking, What Is Your Body Saying ?Document12 pagesBody Language: While You Are Talking, What Is Your Body Saying ?Eng RubaNo ratings yet
- SEC Vs Baguio Country Club CorporationDocument1 pageSEC Vs Baguio Country Club CorporationMaica Mahusay0% (1)
- Aerobes Chapter 12Document6 pagesAerobes Chapter 12Kristine BoholstNo ratings yet
- All Barangay Visitation April 2Document12 pagesAll Barangay Visitation April 2Gina RoseNo ratings yet
- DocuDocument105 pagesDocuKhryss Paula BaldonadoNo ratings yet
- Dwelly Cauley v. United States, 11th Cir. (2010)Document5 pagesDwelly Cauley v. United States, 11th Cir. (2010)Scribd Government DocsNo ratings yet
- ASIL Public International Law Bar Reviewer 2019 PDFDocument73 pagesASIL Public International Law Bar Reviewer 2019 PDFVM50% (2)
- Republic vs. CA 315 SCRA 600Document3 pagesRepublic vs. CA 315 SCRA 600Marianne Shen Petilla100% (1)
- Danial Latifi V. Union of India: Arvind Singh KushwahaDocument5 pagesDanial Latifi V. Union of India: Arvind Singh KushwahaghjegjwNo ratings yet
- Fraud Examination 4th Edition Albrecht Test BankDocument15 pagesFraud Examination 4th Edition Albrecht Test Bankcatfishmabblefeq100% (28)
- The Punjab Local Government Ordinance, 2001Document165 pagesThe Punjab Local Government Ordinance, 2001Rh_shakeelNo ratings yet
- Exclusionary RuleDocument1 pageExclusionary RuleHenry ManNo ratings yet
- Nisce vs. Equitable PCI Bank, Inc.Document30 pagesNisce vs. Equitable PCI Bank, Inc.Lj Anne PacpacoNo ratings yet
- Transfer of PropertyDocument3 pagesTransfer of PropertySaurabh RajNo ratings yet
- English Civil WarDocument48 pagesEnglish Civil WarsmrithiNo ratings yet
- Operating Room Nursing: S Y 2018-2019 FIRST SEMDocument29 pagesOperating Room Nursing: S Y 2018-2019 FIRST SEMMaria Sheila BelzaNo ratings yet
- United States Court of Appeals, Third CircuitDocument80 pagesUnited States Court of Appeals, Third CircuitScribd Government DocsNo ratings yet
- UNOPS General Conditions Goods ENDocument12 pagesUNOPS General Conditions Goods ENMohammedNo ratings yet