You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Usmle Exam Slides!!!Document119 pagesUsmle Exam Slides!!!Tarek Hassouna94% (33)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Arabic PronounsDocument64 pagesArabic Pronounsfatinzalila0% (1)
- Cardiac MRI Made Easy 2008Document164 pagesCardiac MRI Made Easy 2008Benjamin Gonzalez100% (1)
- Pathophysiology of Congestive Heart FailureDocument2 pagesPathophysiology of Congestive Heart FailureAnonymous XvwKtnSrMR100% (10)
- Raminder Nirula - High-Yield Internal Medicine (High-Yield Series) - Lippincott Williams and Wilkins (2006)Document228 pagesRaminder Nirula - High-Yield Internal Medicine (High-Yield Series) - Lippincott Williams and Wilkins (2006)Isah Mohammed100% (1)
- John Chambers, Sandeep S. Hothi, Camelia DemetrescuDocument269 pagesJohn Chambers, Sandeep S. Hothi, Camelia DemetrescuGianina CraiaNo ratings yet
- الباطنة كلها بالتفصيل في 160 صفحة فقط لازم تحمل المذكرة فوراDocument163 pagesالباطنة كلها بالتفصيل في 160 صفحة فقط لازم تحمل المذكرة فورانادين مطر0% (1)
- CARDIOLOGY – “PLABABLE” VALVULAR HEART DISEASE SIGNSDocument22 pagesCARDIOLOGY – “PLABABLE” VALVULAR HEART DISEASE SIGNSTirtha Taposh100% (1)
- Pulmonary EdemaDocument10 pagesPulmonary EdemaNader Smadi100% (6)
- Acr 2016 Dxit Exam Sets - WebDocument129 pagesAcr 2016 Dxit Exam Sets - WebElios NaousNo ratings yet
- 01 - Introduction To Computer and Algorithm - PortalDocument35 pages01 - Introduction To Computer and Algorithm - PortalfatinzalilaNo ratings yet
- Seminar On Rhuematic Heart DiseaseDocument16 pagesSeminar On Rhuematic Heart Diseasenaga maniNo ratings yet
- L07 Destructive Test PDFDocument14 pagesL07 Destructive Test PDFfatinzalila100% (1)
- PLSB Comment Not Done - Cable List Summary & Status ReportDocument26 pagesPLSB Comment Not Done - Cable List Summary & Status ReportfatinzalilaNo ratings yet
- Report To PLSB (Issues & Remarks)Document4 pagesReport To PLSB (Issues & Remarks)fatinzalilaNo ratings yet
- Full Data For Tensile TestDocument10 pagesFull Data For Tensile TestfatinzalilaNo ratings yet
- Final Viva ZalilaDocument51 pagesFinal Viva ZalilafatinzalilaNo ratings yet
- Jadual Kelas Sem 1 Tahun 3Document2 pagesJadual Kelas Sem 1 Tahun 3fatinzalilaNo ratings yet
- CHAPTER 1 Proposal Capstone RWFDocument7 pagesCHAPTER 1 Proposal Capstone RWFfatinzalilaNo ratings yet
- 5 4 18 Obstructions IssuesDocument8 pages5 4 18 Obstructions IssuesfatinzalilaNo ratings yet
- Swelling Test ResultDocument5 pagesSwelling Test ResultfatinzalilaNo ratings yet
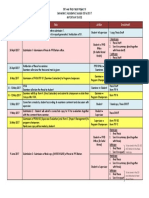
- Important Dates EBT446Document1 pageImportant Dates EBT446fatinzalilaNo ratings yet
- Template Data Swelling TestDocument8 pagesTemplate Data Swelling TestfatinzalilaNo ratings yet
- Advanced Electron Microscopy in The Study of Multimetallic Nanoparticles (Polyol MethodDocument34 pagesAdvanced Electron Microscopy in The Study of Multimetallic Nanoparticles (Polyol MethodfatinzalilaNo ratings yet
- Slide Viva 1 Proposal RWFDocument13 pagesSlide Viva 1 Proposal RWFfatinzalilaNo ratings yet
- L08 Metallography PDFDocument10 pagesL08 Metallography PDFfatinzalilaNo ratings yet
- L09 Distortion Control - PDF - 2Document4 pagesL09 Distortion Control - PDF - 2fatinzalilaNo ratings yet
- L11 Production Welding PDFDocument14 pagesL11 Production Welding PDFfatinzalilaNo ratings yet
- L05 Welding Metallurgy PDFDocument15 pagesL05 Welding Metallurgy PDFfatinzalilaNo ratings yet
- L04 SmawDocument16 pagesL04 SmawfatinzalilaNo ratings yet
- Material Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015Document89 pagesMaterial Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015fatinzalilaNo ratings yet
- L03 Welding Symbols PDFDocument9 pagesL03 Welding Symbols PDFfatinzalilaNo ratings yet
- Material Selection: Case Studies: Materials Selection and Design EBT 447 SEMESTER II, 2013/2014Document37 pagesMaterial Selection: Case Studies: Materials Selection and Design EBT 447 SEMESTER II, 2013/2014fatinzalilaNo ratings yet
- Material Selection & DesignDocument22 pagesMaterial Selection & DesignfatinzalilaNo ratings yet
- Material Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015Document38 pagesMaterial Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015fatinzalilaNo ratings yet
- CHAPTER 1 Proposal Capstone RWFDocument7 pagesCHAPTER 1 Proposal Capstone RWFfatinzalilaNo ratings yet
- Materials The Environment: Ebt 447: Materials Selection and DesignDocument37 pagesMaterials The Environment: Ebt 447: Materials Selection and DesignfatinzalilaNo ratings yet
- Material Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015Document123 pagesMaterial Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015fatinzalilaNo ratings yet
- Materials Selection FundamentalsDocument35 pagesMaterials Selection FundamentalsfatinzalilaNo ratings yet
- Full Report Capstone Senior RWFDocument62 pagesFull Report Capstone Senior RWFfatinzalilaNo ratings yet
- JIPMER 2008-09 Curriculum for Cardiology DM CourseDocument58 pagesJIPMER 2008-09 Curriculum for Cardiology DM Coursefindingnemo667No ratings yet
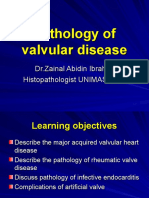
- Pathology of Valvular Disease Version 2009Document65 pagesPathology of Valvular Disease Version 2009lilydariniNo ratings yet
- Radiological Diagnostic of Heart Disease:chest Part 1Document17 pagesRadiological Diagnostic of Heart Disease:chest Part 1rakshit09100% (1)
- Left Atrial Appendage Occlusion For Stroke Prevention in Nonvalvular Atrial Fibrillation 2021Document18 pagesLeft Atrial Appendage Occlusion For Stroke Prevention in Nonvalvular Atrial Fibrillation 2021吳醫師No ratings yet
- Mechanical Heart Valve vs. Bioprosthetic ValveDocument55 pagesMechanical Heart Valve vs. Bioprosthetic ValvePUSHPITHA PERERANo ratings yet
- ESC Guidelines On Cardio-Oncology - 2022Document133 pagesESC Guidelines On Cardio-Oncology - 2022nicolasNo ratings yet
- Diagnostic Tests in CardiologyDocument38 pagesDiagnostic Tests in CardiologyDea Amelia YolandaNo ratings yet
- Example 001Document13 pagesExample 001Priya SelvarajNo ratings yet
- Pash Syndrome Co-Existing With Rheumatic Heart Disease and Severe Mitral Valve Regurgitation: A Rare Case ReportDocument3 pagesPash Syndrome Co-Existing With Rheumatic Heart Disease and Severe Mitral Valve Regurgitation: A Rare Case ReportIJAR JOURNALNo ratings yet
- Heart Valve Disease Treatment Guide - Cleveland ClinicDocument12 pagesHeart Valve Disease Treatment Guide - Cleveland ClinicGuillermo CenturionNo ratings yet
- PUA006 Valve Disease Assessment Poster - Print ReadyDocument1 pagePUA006 Valve Disease Assessment Poster - Print ReadyLuis Fernando Morales JuradoNo ratings yet
- PT Management & Problems of The CV System - Part 4 Cheat SheetDocument2 pagesPT Management & Problems of The CV System - Part 4 Cheat SheetKat KatNo ratings yet
- AHA Card CombinedDocument2 pagesAHA Card CombinedAdrian Gutierrez NajeraNo ratings yet
- Valvular Heart Disease Def PDFDocument3 pagesValvular Heart Disease Def PDFAfif Al BaalbakiNo ratings yet
- Preoperative Assessment. Plauntz (2007)Document17 pagesPreoperative Assessment. Plauntz (2007)Dario Cahuaza :VNo ratings yet
- Icf KardiorespirasiDocument8 pagesIcf KardiorespirasiTahu BulatNo ratings yet
- Diagnostic Tests in CardiologyDocument38 pagesDiagnostic Tests in CardiologyDea Amelia YolandaNo ratings yet
- Hyperemia CongestionDocument40 pagesHyperemia CongestionBikash PuriNo ratings yet
- CVS Path Questions 1Document4 pagesCVS Path Questions 1Vaishali PrasharNo ratings yet
- BSC CardtechDocument25 pagesBSC CardtechShahidriswanNo ratings yet