You might also like
- Karam 2018Document14 pagesKaram 2018Sigit Nian PrasetyoNo ratings yet
- Binahong Leaf Infusion Hand Sanitizer Gel Antibacterial Activity Staphylococcus AureusDocument8 pagesBinahong Leaf Infusion Hand Sanitizer Gel Antibacterial Activity Staphylococcus AureusSigit Nian PrasetyoNo ratings yet
- Jurnal k3Document10 pagesJurnal k3Sigit Nian PrasetyoNo ratings yet
- Formulation and Evaluation of Herbal Hand Sanitizer Using Argemone MexicanaDocument3 pagesFormulation and Evaluation of Herbal Hand Sanitizer Using Argemone MexicanaSigit Nian PrasetyoNo ratings yet
- Durusul Lugatil Arabiyye 1Document127 pagesDurusul Lugatil Arabiyye 1yusuf16360% (5)
- SPO Pengelolaan Pasien Transmisi DropletDocument1 pageSPO Pengelolaan Pasien Transmisi DropletSigit Nian PrasetyoNo ratings yet
- Jurnal k3Document10 pagesJurnal k3Sigit Nian PrasetyoNo ratings yet
- Motivational Factors of Hospital EmployeesDocument19 pagesMotivational Factors of Hospital EmployeesSigit Nian PrasetyoNo ratings yet
- SPO Alur Pelayanan Pasien TB Di Rawat InapDocument1 pageSPO Alur Pelayanan Pasien TB Di Rawat InapSigit Nian PrasetyoNo ratings yet
- SPO Triase Pasien Batuk Dirawat Jalan PDFDocument1 pageSPO Triase Pasien Batuk Dirawat Jalan PDFSigit Nian PrasetyoNo ratings yet
- SPO Triase Pasien Batuk Dirawat JalanDocument1 pageSPO Triase Pasien Batuk Dirawat JalanSigit Nian PrasetyoNo ratings yet
- SPO Pemulangan Pasien InfeksiusDocument1 pageSPO Pemulangan Pasien InfeksiusSigit Nian PrasetyoNo ratings yet
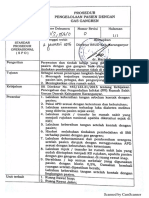
- SPO Pengelolaan Pasien DGN Gas GangrenDocument1 pageSPO Pengelolaan Pasien DGN Gas GangrenSigit Nian PrasetyoNo ratings yet
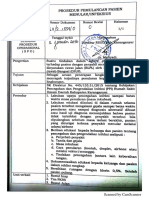
- SPO Prosedur Penanganan Pasien Hiv PDFDocument1 pageSPO Prosedur Penanganan Pasien Hiv PDFSigit Nian PrasetyoNo ratings yet
- SPO Pengelolaan Pasien Immunosupresif PDFDocument2 pagesSPO Pengelolaan Pasien Immunosupresif PDFSigit Nian PrasetyoNo ratings yet
- SPO Pemulangan Pasien InfeksiusDocument1 pageSPO Pemulangan Pasien InfeksiusSigit Nian PrasetyoNo ratings yet
- Anesthetic Preconditioning: An Anesthesiologist's TaleDocument5 pagesAnesthetic Preconditioning: An Anesthesiologist's TaleSigit Nian PrasetyoNo ratings yet
- Kebijakan Ruang IsolasiDocument6 pagesKebijakan Ruang IsolasiSigit Nian PrasetyoNo ratings yet
- Cataract Surgeries: Health at A Glance 2011Document4 pagesCataract Surgeries: Health at A Glance 2011Sigit Nian PrasetyoNo ratings yet
- SPO Prosedur Penanganan Pasien HivDocument1 pageSPO Prosedur Penanganan Pasien HivSigit Nian PrasetyoNo ratings yet
- Insiden Prevalensi AIDSDocument4 pagesInsiden Prevalensi AIDSSigit Nian PrasetyoNo ratings yet
- Premature Mortality: Health at A Glance 2011Document4 pagesPremature Mortality: Health at A Glance 2011Sigit Nian PrasetyoNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Transes Anaphy LEC (INTRO TO ANATOMY)Document6 pagesTranses Anaphy LEC (INTRO TO ANATOMY)Reign SaplacoNo ratings yet
- Emergency and Disaster NursingDocument13 pagesEmergency and Disaster Nursingkarenkaren09No ratings yet
- Endometrial Study by TVS and It's Correlation With Histopathology in Abnormal Uterine BleedingDocument12 pagesEndometrial Study by TVS and It's Correlation With Histopathology in Abnormal Uterine BleedingIOSRjournalNo ratings yet
- Snow White - Abnormal Psychology PaperDocument6 pagesSnow White - Abnormal Psychology PaperNicky JosephNo ratings yet
- Nejm 2204556Document11 pagesNejm 2204556tommy taylor084No ratings yet
- Dickens and Bio Politics. ArticleDocument24 pagesDickens and Bio Politics. ArticleJose Luis FernandezNo ratings yet
- Case Study 3 WorduDocument5 pagesCase Study 3 WorduMelissa Andrea JajallaNo ratings yet
- Tiens Food Supplements CatalogueDocument26 pagesTiens Food Supplements CatalogueWahyu TriArya Budhi ChrissantyoNo ratings yet
- HSV 2 TreatmentDocument23 pagesHSV 2 Treatmentbobhelp100% (1)
- Cancer DiseaseDocument7 pagesCancer Diseasenbs saraswathiNo ratings yet
- Family Case Study of the Bucasas FamilyDocument27 pagesFamily Case Study of the Bucasas FamilyKristel AnneNo ratings yet
- 1 Septicemia, & SepsisDocument14 pages1 Septicemia, & SepsisfgrNo ratings yet
- Newborn Resuscitation Program (NRP) TechniquesDocument47 pagesNewborn Resuscitation Program (NRP) TechniquesNethera Kiza ImperialNo ratings yet
- Hesi Hints Part 4Document2 pagesHesi Hints Part 4Sharon TanveerNo ratings yet
- EAU Pocket Guideline 2021Document525 pagesEAU Pocket Guideline 2021Maria Angelica Rodriguez100% (1)
- DR Kiki Lukman Patofisiologi Acute CholangitisDocument36 pagesDR Kiki Lukman Patofisiologi Acute CholangitisAfkar30No ratings yet
- Higher Order Thinking Skills (HOTS) Questions: Grade 10: ScienceDocument3 pagesHigher Order Thinking Skills (HOTS) Questions: Grade 10: Sciencesahil ahmedNo ratings yet
- Apoptosis & Its Relation To CancerDocument16 pagesApoptosis & Its Relation To CancerRohan DuttaNo ratings yet
- PSM 2 PypDocument186 pagesPSM 2 PypsuriNo ratings yet
- Marvin L.-Gen Ed-QuestionDocument14 pagesMarvin L.-Gen Ed-QuestionALJa bherNo ratings yet
- Lesson PlanDocument10 pagesLesson PlanalishaNo ratings yet
- Nervous System WorksheetDocument3 pagesNervous System WorksheetaNo ratings yet
- Pembagian PPK Elektif OrthoDocument4 pagesPembagian PPK Elektif OrthoIbnu ImadudinNo ratings yet
- Video Recap of Alleles and Genes by Amoeba SistersDocument3 pagesVideo Recap of Alleles and Genes by Amoeba Sistersur100% (2)
- 10 11648 J Ijde 20200502 12Document4 pages10 11648 J Ijde 20200502 12AdemoluNo ratings yet
- Neuromuscular Blocking DrugsDocument23 pagesNeuromuscular Blocking DrugsRA TranceNo ratings yet
- 5 Common Tennis Injuries and 4 Ways To Prevent ThemDocument4 pages5 Common Tennis Injuries and 4 Ways To Prevent ThemTitser AyMiNo ratings yet
- Pharmacotherapy DipiroDocument70 pagesPharmacotherapy DipiroSisisNo ratings yet
- Surgical Treatment of Tarsal Coalitions in ChildrenDocument10 pagesSurgical Treatment of Tarsal Coalitions in ChildrenNegru TeodorNo ratings yet
- Reading and Writing: Quarter 3: Module 2 - Lesson 1Document13 pagesReading and Writing: Quarter 3: Module 2 - Lesson 1MELANIE IBARDALOZA100% (2)