You might also like
- The COAT & Review Approach: How to recognise and manage unwell patientsFrom EverandThe COAT & Review Approach: How to recognise and manage unwell patientsRating: 5 out of 5 stars5/5 (1)
- Introduction To Nursing: Pamela M. Llana, MSN, RNDocument40 pagesIntroduction To Nursing: Pamela M. Llana, MSN, RNhelen brock100% (1)
- Unit 8 Career PlanningDocument7 pagesUnit 8 Career PlanningVishnu LataNo ratings yet
- Records and ReportDocument4 pagesRecords and ReportAnusikta PandaNo ratings yet
- Emergency DepartmentDocument25 pagesEmergency DepartmentphanikrNo ratings yet
- Nursing As A Profession: Agung Setiyadi Middle East UniversityDocument33 pagesNursing As A Profession: Agung Setiyadi Middle East UniversityNise Mon KuriakoseNo ratings yet
- Quality Standards For Health Care Organization Patients RightsDocument6 pagesQuality Standards For Health Care Organization Patients RightsLey EnhaimaNo ratings yet
- Professional OrganisationsDocument19 pagesProfessional OrganisationsMonika100% (1)
- Treatment, Prevention and Control of Intestinal Parasitic InfectionDocument49 pagesTreatment, Prevention and Control of Intestinal Parasitic InfectiononilaNo ratings yet
- 2 Infection ControlDocument34 pages2 Infection ControlMustapha S. MintehNo ratings yet
- Lesson Plan Fonn S.1Document10 pagesLesson Plan Fonn S.1Sandeep MeenaNo ratings yet
- Career Planning: Minu Mathew Neeraj VijayDocument14 pagesCareer Planning: Minu Mathew Neeraj Vijayminuannapoovelil7642No ratings yet
- Objective Structured Clinical Examination (OSCE) : Perceptions of Nursing Students in Tuberculosis DiagnosisDocument8 pagesObjective Structured Clinical Examination (OSCE) : Perceptions of Nursing Students in Tuberculosis DiagnosisIJAERS JOURNAL100% (1)
- Lesson Plan On: DocumentationDocument8 pagesLesson Plan On: DocumentationNehaNo ratings yet
- Medication Errors 19 Sep15Document36 pagesMedication Errors 19 Sep15drbharatmalhotr195No ratings yet
- Coordination As A Management FunctionDocument5 pagesCoordination As A Management FunctionanushavergheseNo ratings yet
- Planning, Designing, Functions & Management OF: Anesthesia DepartmentDocument20 pagesPlanning, Designing, Functions & Management OF: Anesthesia Departmentlokitoka zigNo ratings yet
- Methods of Performance Appraisal IDocument8 pagesMethods of Performance Appraisal IRaja SekaranNo ratings yet
- Factors Related To Health PromotionDocument25 pagesFactors Related To Health PromotionKillian SibzNo ratings yet
- Risk Management & Legal IssuesDocument27 pagesRisk Management & Legal IssuesEman RajpootNo ratings yet
- Kharadar General Hospital School of Nursing Manual Fundamental of Nursing Procedures 4-Year BSC NursingDocument31 pagesKharadar General Hospital School of Nursing Manual Fundamental of Nursing Procedures 4-Year BSC NursingJosepheen RajaNo ratings yet
- 1040 Inventory Control Condemnation ProceduresDocument44 pages1040 Inventory Control Condemnation ProceduresnagssaraNo ratings yet
- Formulation of Philosophy and Objectives: Prepared By: Ms. Sameeksha Nursing Tutor ACNDocument34 pagesFormulation of Philosophy and Objectives: Prepared By: Ms. Sameeksha Nursing Tutor ACNDiksha chaudharyNo ratings yet
- Ethical Issues in Nursing PracticeDocument10 pagesEthical Issues in Nursing PracticeP'Babe Cece Adumoah0% (1)
- Paediatric and Neonatal Service and Clinical Quality IndicatorsDocument8 pagesPaediatric and Neonatal Service and Clinical Quality IndicatorsSyamsul Arifin100% (1)
- Nursing ProcessDocument5 pagesNursing Processanimesh pandaNo ratings yet
- Introduction To NutritionDocument19 pagesIntroduction To Nutritionseanne kskwkwkaNo ratings yet
- Documenting ConferringDocument40 pagesDocumenting ConferringDidik Atmojo0% (1)
- Introduction To Nursing ManagementDocument19 pagesIntroduction To Nursing ManagementMUTHUKUMARAN100% (1)
- B M W M: IO Edical Aste AnagementDocument23 pagesB M W M: IO Edical Aste AnagementJishnu JohnNo ratings yet
- Responsibilities and AccountabilityDocument26 pagesResponsibilities and AccountabilityRadha SriNo ratings yet
- Quality AssuranceDocument43 pagesQuality Assurancekanika100% (1)
- Format For Periodical Report On Anti Ragging 2016 17Document3 pagesFormat For Periodical Report On Anti Ragging 2016 17anbuelectricalNo ratings yet
- Quotation For Books in Nursing CollegeDocument12 pagesQuotation For Books in Nursing CollegeIshfaq LoneNo ratings yet
- LeptospirosisDocument12 pagesLeptospirosisKim NichiNo ratings yet
- Laws and Rules Governing HospitalsDocument6 pagesLaws and Rules Governing HospitalsAnil BgNo ratings yet
- Nursing ProcessDocument52 pagesNursing ProcessDzon LornaNo ratings yet
- Performance AppraisalDocument37 pagesPerformance AppraisalBoogie AbellanosaNo ratings yet
- Reference Writing Styles: Mrs. Monika Sharma Lecturer, DMCH, CON, Ludhiana. PunjabDocument82 pagesReference Writing Styles: Mrs. Monika Sharma Lecturer, DMCH, CON, Ludhiana. PunjabNavpreet KaurNo ratings yet
- Family Case Study FormatDocument3 pagesFamily Case Study FormatkasjdkasNo ratings yet
- ResearchDocument80 pagesResearchRamesh RamuNo ratings yet
- Define Medical Audit. Describe The Conditions, Prerequisites & Steps For Conducting Medical Audit in A General HospitalDocument15 pagesDefine Medical Audit. Describe The Conditions, Prerequisites & Steps For Conducting Medical Audit in A General HospitalAbdul RahamanNo ratings yet
- CNO Professional Misconduct - StudentDocument30 pagesCNO Professional Misconduct - StudentdanushaNo ratings yet
- Nabh Tertiary CareDocument7 pagesNabh Tertiary CareGold PANDINo ratings yet
- Medication - errors хорошая перезентацияDocument65 pagesMedication - errors хорошая перезентацияAlina PetichenkoNo ratings yet
- Electroencephalography: Preparation of Patients and Assisting With EEGDocument15 pagesElectroencephalography: Preparation of Patients and Assisting With EEGPaul MNo ratings yet
- Minorailments: Saddam Hussain Lecturer Winm, BharuchDocument46 pagesMinorailments: Saddam Hussain Lecturer Winm, Bharuchsaddam hussain100% (1)
- Family Care StudyDocument13 pagesFamily Care StudyLavanya ChNo ratings yet
- How To Write An Incident ReportDocument5 pagesHow To Write An Incident ReportMelody B. MiguelNo ratings yet
- Module 1 To 4Document208 pagesModule 1 To 4smbawasainiNo ratings yet
- The 5 Nursing Process StepsDocument124 pagesThe 5 Nursing Process StepsEstrera Ruschelle A.No ratings yet
- Emergency & Disaster ManagementDocument39 pagesEmergency & Disaster ManagementSanket Telang100% (1)
- Surveillance Prevention and Control of Infection PlanDocument11 pagesSurveillance Prevention and Control of Infection Plansony kurniawanNo ratings yet
- Revised SNCU Mentoring ChecklistDocument6 pagesRevised SNCU Mentoring Checklistrani26octNo ratings yet
- Triage: Blessy Susan BabuDocument21 pagesTriage: Blessy Susan BabuBlessy SusanNo ratings yet
- Master Rotation Plan For GNMDocument9 pagesMaster Rotation Plan For GNMAnanya HatiNo ratings yet
- 2.SociologyChild AbuseDocument7 pages2.SociologyChild Abusedew23No ratings yet
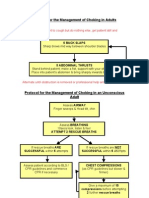
- Protocol For The Management of Choking in AdultsDocument3 pagesProtocol For The Management of Choking in AdultsSarinah RynaNo ratings yet
- Management of A Violent PatientDocument11 pagesManagement of A Violent Patientkingpin@mailinatorNo ratings yet
- Deworming: Fit For SchoolDocument9 pagesDeworming: Fit For SchoolLark SantiagoNo ratings yet
- DRUG STUDY Durano Aireen E.Document4 pagesDRUG STUDY Durano Aireen E.Doneva Lyn MedinaNo ratings yet
- CHPPM How To Write and Exercise PrescriptionDocument160 pagesCHPPM How To Write and Exercise PrescriptionJackie NepomucenoNo ratings yet
- Tarun Kumar ReportDocument1 pageTarun Kumar Reportnavdeep madheshiyaNo ratings yet
- Harjïa, H. C. L. (0 1 ) - Sfjdldhïa Hckcral (:a. CM.) - Japïtuld:, Páhfka : A 8 . Oæxfjd, M.E., OR7 Lardussc - Hrupd Cmftdrfal Atrfa. Pcjupcramd MCDocument7 pagesHarjïa, H. C. L. (0 1 ) - Sfjdldhïa Hckcral (:a. CM.) - Japïtuld:, Páhfka : A 8 . Oæxfjd, M.E., OR7 Lardussc - Hrupd Cmftdrfal Atrfa. Pcjupcramd MCSofia PerezNo ratings yet
- Strong: Nutritional Risk Screening Tool For Children Aged Month - 18 Years On Admission To The HospitalDocument3 pagesStrong: Nutritional Risk Screening Tool For Children Aged Month - 18 Years On Admission To The HospitalninaNo ratings yet
- Arthur Steindler: Pes Cavus (1921), He Analyzed The Muscle ImbalDocument3 pagesArthur Steindler: Pes Cavus (1921), He Analyzed The Muscle Imbalisaac b-127No ratings yet
- Epidemology TestDocument12 pagesEpidemology TestS.100% (1)
- Limfoma Kutis Pada Pasien Yang Semula Di DiagnosisDocument34 pagesLimfoma Kutis Pada Pasien Yang Semula Di DiagnosisChris MulyoNo ratings yet
- Congenital DiseaseDocument39 pagesCongenital DiseaseRavi SharmaNo ratings yet
- Lumbar Fusion and DebracingDocument4 pagesLumbar Fusion and DebracingDina Lutfy SharafNo ratings yet
- Forward IMRT Breast PDFDocument54 pagesForward IMRT Breast PDFmitza05100% (1)
- 26071-100-G70-GHX-00071-113 HSE Weekly Report (25 Mar - 31 Mar 2022)Document5 pages26071-100-G70-GHX-00071-113 HSE Weekly Report (25 Mar - 31 Mar 2022)Dwi Agung AriyonoNo ratings yet
- DISSociative AnaesthesiaDocument3 pagesDISSociative Anaesthesiamohit jainNo ratings yet
- Audit On BFHIDocument40 pagesAudit On BFHIYoung MilkNo ratings yet
- Bad Pharma - A Fraud in Clinical Trail DataDocument27 pagesBad Pharma - A Fraud in Clinical Trail DataSimran WaghelaNo ratings yet
- Module-II Day-9Document8 pagesModule-II Day-9HomeoDr Babar AminNo ratings yet
- OligodendrogliomaDocument9 pagesOligodendrogliomaroni pahleviNo ratings yet
- BodyBallancer Lipo Brochure PDFDocument2 pagesBodyBallancer Lipo Brochure PDFRoss Gale100% (1)
- Medical Equipment Technology I: Joseph Asamoah-AsareDocument22 pagesMedical Equipment Technology I: Joseph Asamoah-AsareNyuori CosmasNo ratings yet
- Presentation On Postpartum ComplicationsDocument24 pagesPresentation On Postpartum ComplicationsBeulah DasariNo ratings yet
- Communicable Disease - Community Health NursingDocument49 pagesCommunicable Disease - Community Health Nursinggelean payod100% (1)
- Brown (2001) PDFDocument13 pagesBrown (2001) PDFAna Catarina InácioNo ratings yet
- 14-Antiameobic Antifungal 2021Document22 pages14-Antiameobic Antifungal 2021Amr SalemNo ratings yet
- Hematology Cell Morphology ChartDocument2 pagesHematology Cell Morphology ChartMiaoNo ratings yet
- Service Annotated BibliographyDocument6 pagesService Annotated Bibliographyapi-355966257No ratings yet
- Skin Premalignant and TumorsDocument95 pagesSkin Premalignant and TumorsmedicoprakashNo ratings yet
- Psychiatric Assessment Scale InfoDocument2 pagesPsychiatric Assessment Scale InfoRoxana SanduNo ratings yet
- Elman Book FlyerDocument2 pagesElman Book FlyerCarolina CruzNo ratings yet
- Fs 15Document8 pagesFs 15api-299490997No ratings yet