You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Fungal Infection 22Document11 pagesFungal Infection 22sazaki224No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- GenetDocument47 pagesGenet88AKKNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Lecture MMMMMDocument77 pagesLecture MMMMMsazaki224No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Introduction To PharmacogenomicsDocument35 pagesIntroduction To Pharmacogenomicssazaki224No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 100 FactsDocument109 pages100 FactsWintershadeNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Introduction To PharmacogenomicsDocument35 pagesIntroduction To Pharmacogenomicssazaki224No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Chapter15 ModifiedDocument19 pagesChapter15 Modifiedsazaki224No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Drugmetabolism 130121005951 Phpapp01Document69 pagesDrugmetabolism 130121005951 Phpapp01sazaki224No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Organizationofhospitalpharmacyslides 140714113548 Phpapp01Document27 pagesOrganizationofhospitalpharmacyslides 140714113548 Phpapp01sazaki224No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Claudia K As SerraDocument17 pagesClaudia K As Serrasazaki224No ratings yet
- Genomics GeneticsDocument40 pagesGenomics Geneticssazaki224No ratings yet
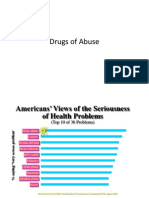
- Drugs of AbuseDocument71 pagesDrugs of Abusesazaki224No ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Autacoides LectureDocument20 pagesAutacoides Lecturesazaki224No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Autacoides LectureDocument20 pagesAutacoides Lecturesazaki224No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hepatorenal SyndromeDocument1 pageHepatorenal Syndromesazaki224No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Systemic Lupus Erythematosus PDFDocument4 pagesSystemic Lupus Erythematosus PDFsazaki224No ratings yet
- Basic Radiation BiologyDocument25 pagesBasic Radiation Biologysazaki224No ratings yet
- CaVital WRC - BroshureDocument12 pagesCaVital WRC - Broshuresazaki224No ratings yet
- Famillial HypercholesterolemiaDocument9 pagesFamillial Hypercholesterolemiasazaki224No ratings yet
- Pregnancy and Breast-Feeding: Mosby Items and Derived Items © 2007 by Mosby, Inc., An Affiliate of Elsevier IncDocument10 pagesPregnancy and Breast-Feeding: Mosby Items and Derived Items © 2007 by Mosby, Inc., An Affiliate of Elsevier Incsazaki224No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 23 Drugs For Emergencies QuestionsDocument6 pages23 Drugs For Emergencies Questionssazaki224No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- 24 Contraceptives QuestionsDocument6 pages24 Contraceptives Questionssazaki224No ratings yet
- Pregnancy and Breast-Feeding: Mosby Items and Derived Items © 2007 by Mosby, Inc., An Affiliate of Elsevier IncDocument10 pagesPregnancy and Breast-Feeding: Mosby Items and Derived Items © 2007 by Mosby, Inc., An Affiliate of Elsevier Incsazaki224No ratings yet
- PsychopharmacologyDocument49 pagesPsychopharmacologysazaki224No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 25 Drug Interactions QuestionsDocument7 pages25 Drug Interactions Questionssazaki22483% (6)
- Antiviral Drugs: An Overview: Chris Brooks CHEM 5398 Medicinal Chemistry Prof. BuynakDocument18 pagesAntiviral Drugs: An Overview: Chris Brooks CHEM 5398 Medicinal Chemistry Prof. BuynakShweta NimwalNo ratings yet
- PsychopharmacologyDocument49 pagesPsychopharmacologysazaki224No ratings yet
- PsychopharmacologyDocument49 pagesPsychopharmacologysazaki224No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- 23 Drugs For EmergenciesDocument11 pages23 Drugs For Emergenciessazaki224No ratings yet
- Causes and Symptoms of High FeverDocument4 pagesCauses and Symptoms of High Feverblah4044No ratings yet
- 11805001Document2 pages11805001Aniket DubeyNo ratings yet
- Vasculitis in Juvenile-Onset Systemic Lupus Erythematosus: Eve M. D. Smith, Hanna Lythgoe and Christian M. HedrichDocument9 pagesVasculitis in Juvenile-Onset Systemic Lupus Erythematosus: Eve M. D. Smith, Hanna Lythgoe and Christian M. HedrichMaya SusantiNo ratings yet
- Adipogenesis and Metabolic Health PDFDocument17 pagesAdipogenesis and Metabolic Health PDFalbertoNo ratings yet
- Full Download Test Bank For Comprehensive Radiographic Pathology 6th Edition by Eisenberg PDF Full ChapterDocument36 pagesFull Download Test Bank For Comprehensive Radiographic Pathology 6th Edition by Eisenberg PDF Full Chapterdiesnongolgothatsczx100% (13)
- Curier Nr4.indd PDFDocument58 pagesCurier Nr4.indd PDFCristinaCaprosNo ratings yet
- The 3500-Year History of Alopecia Areata ResearchDocument24 pagesThe 3500-Year History of Alopecia Areata ResearchmedifacuNo ratings yet
- Guyabano Herbal MedicineDocument8 pagesGuyabano Herbal MedicineJosua GarciaNo ratings yet
- Chapter 24:: Allergic Contact Dermatitis:: Jake E. Turrentine, Michael P. SheehanDocument19 pagesChapter 24:: Allergic Contact Dermatitis:: Jake E. Turrentine, Michael P. SheehanInke LubisNo ratings yet
- Infectious Disease I - 14 (1) - Severe Sepsis and Septic Shock (Courses in Therapeutics and Disease State Management)Document35 pagesInfectious Disease I - 14 (1) - Severe Sepsis and Septic Shock (Courses in Therapeutics and Disease State Management)Ali AlyahawiNo ratings yet
- CRP LX High Sensitive enDocument4 pagesCRP LX High Sensitive enLince WijoyoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Muscular System Disease (Myositis)Document17 pagesMuscular System Disease (Myositis)siti nurfadhilahNo ratings yet
- Dermatology ResearchDocument9 pagesDermatology ResearchjumaracruzNo ratings yet
- Anatomy and Physiology Immune System OverviewDocument50 pagesAnatomy and Physiology Immune System OverviewIrumvamwizerwa OnesmeNo ratings yet
- Musculoskeletal Physiotherapy: Treating InjuriesDocument35 pagesMusculoskeletal Physiotherapy: Treating InjuriesRaluca AndreeaNo ratings yet
- Asthma Thesis StatementDocument4 pagesAsthma Thesis Statementfjnev0hc100% (2)
- Necrotizing Enterocolitis Pathophysiology InsightsDocument21 pagesNecrotizing Enterocolitis Pathophysiology InsightsdenisNo ratings yet
- Microbiology Objective QuestionsDocument28 pagesMicrobiology Objective QuestionscrazybobblaskeyNo ratings yet
- Photobiomodulation - An Invaluable Tool For All Dental SpecialtiesDocument8 pagesPhotobiomodulation - An Invaluable Tool For All Dental SpecialtiessillyazianNo ratings yet
- Chamomile PDFDocument21 pagesChamomile PDFSebastian NemethNo ratings yet
- DRUG STUDY CLOBETASOL CREAMrevisedDocument2 pagesDRUG STUDY CLOBETASOL CREAMrevisedswitchlers anneNo ratings yet
- AutoimmuneSolution FINALDocument24 pagesAutoimmuneSolution FINALadyro12100% (1)
- CopdDocument4 pagesCopdapi-3739910100% (2)
- Granuloma TuberculosisDocument9 pagesGranuloma TuberculosisÁlvaro Alexandro Morales JiménezNo ratings yet
- Bioquimica de La Isquemia y Reperfusion ArticuloDocument35 pagesBioquimica de La Isquemia y Reperfusion ArticulofelipeNo ratings yet
- Wound Essentials 5 Investigating Wound InfectionDocument5 pagesWound Essentials 5 Investigating Wound Infectionyash agarwalNo ratings yet
- 2033 Rheumatoid Arthritis 14-1 PDFDocument48 pages2033 Rheumatoid Arthritis 14-1 PDFAfif Al FatihNo ratings yet
- Morpho - Pathology Final Summary: Chapter 1: Cellular Reactions To AggressionDocument21 pagesMorpho - Pathology Final Summary: Chapter 1: Cellular Reactions To Aggressiondjxela89No ratings yet
- Rietz Thyroid Final PDFDocument50 pagesRietz Thyroid Final PDFRoberto CortezNo ratings yet
- Pithecellobium Dulce (Roxb.) Benth.: Sweet TamarindDocument15 pagesPithecellobium Dulce (Roxb.) Benth.: Sweet TamarindMay EvelynNo ratings yet