You might also like
- 5 Steps To Give Her Screaming Hip Shaking OrgasmsDocument24 pages5 Steps To Give Her Screaming Hip Shaking OrgasmsBright Williams Boakye27% (11)
- PEDIATRIC Endocrinology MCQDocument5 pagesPEDIATRIC Endocrinology MCQcataztropher75% (12)
- Paeds Short Answer QuestionsDocument2 pagesPaeds Short Answer Questionsgokubardock88% (8)
- Neonatology MCQDocument34 pagesNeonatology MCQNadeem Ur Rasool Sahibzada94% (31)
- Neonatology Mock Exam 6 PDFDocument6 pagesNeonatology Mock Exam 6 PDFMostafa Mahmoud Elsebey100% (2)
- Pediatrics 100Q AnsweredDocument16 pagesPediatrics 100Q AnsweredMobin Ur Rehman Khan100% (1)
- Pediatric Endocrinology Review MCQsDocument104 pagesPediatric Endocrinology Review MCQsTirou100% (1)
- MCQDocument103 pagesMCQNarendra Saini100% (1)
- Fetus & Neoborn-3Document25 pagesFetus & Neoborn-3Mateen Shukri100% (1)
- ALL Pediatrics End-Block MCQsDocument18 pagesALL Pediatrics End-Block MCQsSarwar Sarkawt100% (1)
- MCQs in PediatricsDocument4 pagesMCQs in Pediatricsarun babu93% (15)
- Neonatology QuestionsDocument8 pagesNeonatology Questionsjaneeydia75% (4)
- MCQ PediatricsDocument7 pagesMCQ PediatricsNasim Shakhshir67% (6)
- Nephrology MCQSDocument16 pagesNephrology MCQSThana AlAnsari100% (5)
- CatheterizationDocument31 pagesCatheterizationAlfi Nur Hanifah100% (1)
- Pediatric Robotic SurgeryDocument188 pagesPediatric Robotic SurgeryPablo Lukacs CarmonaNo ratings yet
- 5th Year 112 PediatricsDocument12 pages5th Year 112 PediatricsAmjad A. Amir100% (2)
- Newborn MCQDocument58 pagesNewborn MCQعبدالرحمن بشير100% (2)
- Pedes McqsDocument16 pagesPedes McqsSyeda Aroosa Abbas Naqvi100% (1)
- Pediatrics Objective Type Questions and Answers - All Medical Questions and AnswersDocument4 pagesPediatrics Objective Type Questions and Answers - All Medical Questions and AnswersAbdul Ghaffar AbdullahNo ratings yet
- Soal MCQDocument39 pagesSoal MCQRonald Allan Valle SantosNo ratings yet
- Mcqforneonatology 120612005106 Phpapp02Document7 pagesMcqforneonatology 120612005106 Phpapp02DoctorSajid BuzdarNo ratings yet
- Pediatrics Question PaperDocument21 pagesPediatrics Question Paperprinceej100% (3)
- All Pediatrics 2Document200 pagesAll Pediatrics 2niemand daNo ratings yet
- Name: - Date: - Date of Rotation: - Score: - Pediatrics Shifting ExamDocument5 pagesName: - Date: - Date of Rotation: - Score: - Pediatrics Shifting ExamKristine Seredrica100% (1)
- اذكرونا بدعوة Pediatric Theory Final ExamDocument23 pagesاذكرونا بدعوة Pediatric Theory Final ExamSarwar Sarkawt100% (1)
- Filename: AMC PEDIATRICS 2005 To 2009 PDFDocument38 pagesFilename: AMC PEDIATRICS 2005 To 2009 PDFZahid QamarNo ratings yet
- First Part Exam - Feb 2020Document16 pagesFirst Part Exam - Feb 2020hassan mohamedNo ratings yet
- Preps A 2009Document830 pagesPreps A 2009Rita Maya HaddadNo ratings yet
- Khalid Alfaki PedDocument21 pagesKhalid Alfaki PedAli HusseinNo ratings yet
- NeomcqDocument32 pagesNeomcqSyeda Aroosa Abbas NaqviNo ratings yet
- 2014 Final Paediatric Exam (تم الحفظ تلقائيًا)Document258 pages2014 Final Paediatric Exam (تم الحفظ تلقائيًا)wea xcz100% (4)
- (PAED) End-Posting Examination Questions (R3G1)Document16 pages(PAED) End-Posting Examination Questions (R3G1)loxNo ratings yet
- Pedia Super Samplex 2Document50 pagesPedia Super Samplex 2Sheryl Layne LaoNo ratings yet
- 4 5839111053702598026Document7 pages4 5839111053702598026خلدون سليمNo ratings yet
- Pediatrics BookDocument53 pagesPediatrics BookMobin Ur Rehman Khan100% (1)
- Mcqs PediatricsDocument155 pagesMcqs PediatricsAhmed Kh. Abu Warda100% (1)
- Paediatric Question BankDocument27 pagesPaediatric Question BankBashiru SelemaniNo ratings yet
- Part C-35 MCQS/ 7 PP: MCQ PaediatricsDocument6 pagesPart C-35 MCQS/ 7 PP: MCQ Paediatricswindows3123100% (1)
- Pediatrics Problem Solving QsDocument32 pagesPediatrics Problem Solving QsabozinaNo ratings yet
- Ped A Internship 1517300917 PDF 2Document13 pagesPed A Internship 1517300917 PDF 2dariasuslowaNo ratings yet
- BXX - Pediatrics PDocument57 pagesBXX - Pediatrics PJason Steel100% (1)
- Pediatrics PG Exam PapersDocument39 pagesPediatrics PG Exam Paperscooldude_secbad1712100% (1)
- Transposition of The Great ArteriesDocument23 pagesTransposition of The Great Arterieswaseem mohammedNo ratings yet
- Bawasig Pediatric ExamDocument20 pagesBawasig Pediatric Examخلدون سليمNo ratings yet
- Pedia QDocument36 pagesPedia QAmal100% (1)
- Pediatric 6th Year 2016Document30 pagesPediatric 6th Year 2016motasem alsharifNo ratings yet
- Mbbs Final Professional Examination 2007 Paediatric Medicine (MCQS)Document8 pagesMbbs Final Professional Examination 2007 Paediatric Medicine (MCQS)Muhammad Bilal100% (1)
- Pediatric QuestionDocument11 pagesPediatric QuestionDana ChernovNo ratings yet
- PEDIA DOCUMENT REVIEWDocument157 pagesPEDIA DOCUMENT REVIEWBea Y. Bas-ong100% (1)
- MK Paeds BazookaDocument118 pagesMK Paeds BazookaChipasha Bwalya100% (1)
- Pediatric Q&ADocument12 pagesPediatric Q&AMateen ShukriNo ratings yet
- Aap 2009Document538 pagesAap 2009toniassaf100% (1)
- Paeds MCQs Part 1Document34 pagesPaeds MCQs Part 1SsNo ratings yet
- Aapprep2009 141022094533 Conversion Gate01 PDFDocument847 pagesAapprep2009 141022094533 Conversion Gate01 PDFAndrew SidhuNo ratings yet
- Nutrition Board ReviewDocument52 pagesNutrition Board ReviewWaleed AlakbariNo ratings yet
- Infant Jaundice, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandInfant Jaundice, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Nbme 2 Block 1-4Document112 pagesNbme 2 Block 1-4lk0704No ratings yet
- NBME 2 Block 1-4 EditedDocument83 pagesNBME 2 Block 1-4 EditedنبيلالمسلاتيNo ratings yet
- NBME 2 Block 1-4 All IncludedDocument112 pagesNBME 2 Block 1-4 All Included3592648No ratings yet
- NBME 2 BlocksDocument112 pagesNBME 2 Blocks3592648No ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant SurgeonDocument65 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant SurgeonEslam R. Almassri100% (1)
- 8 - WoundDocument13 pages8 - WoundEslam R. AlmassriNo ratings yet
- Examination FinalDocument36 pagesExamination FinalEslam R. AlmassriNo ratings yet
- 0000000Document20 pages0000000Eslam R. AlmassriNo ratings yet
- Q1Document18 pagesQ1Eslam R. AlmassriNo ratings yet
- صحمستند+MicDocument17 pagesصحمستند+MicLemar AhmedNo ratings yet
- MedicineDocument409 pagesMedicineFaizur RahmanNo ratings yet
- Ear AnatomyDocument100 pagesEar AnatomyEslam R. AlmassriNo ratings yet
- IUGA Scoring SystemDocument40 pagesIUGA Scoring SystemBudi Iman SantosoNo ratings yet
- Patent US6447462Document15 pagesPatent US6447462Yodi SoebadiNo ratings yet
- Pain in The Throne: Cristal Ann Laquindanum TMC ER RotationDocument39 pagesPain in The Throne: Cristal Ann Laquindanum TMC ER RotationAkhil SunkariNo ratings yet
- Sexually Transmitted Infections PowerpointDocument12 pagesSexually Transmitted Infections Powerpointkriss ellisNo ratings yet
- HypospadiasDocument12 pagesHypospadiasLeni LukmanNo ratings yet
- NephrolithiasisDocument2 pagesNephrolithiasisDeepthiNo ratings yet
- TURP Procedure Guide for Prostate RemovalDocument4 pagesTURP Procedure Guide for Prostate RemovalJylme Keziah Manzano DoronioNo ratings yet
- A Century of Prostatic SurgeryDocument7 pagesA Century of Prostatic SurgeryLjubomirErdoglijaNo ratings yet
- Male Reproductive Anatomy and Physiology: 1. PenisDocument7 pagesMale Reproductive Anatomy and Physiology: 1. PenisMhiahLine TolentinoNo ratings yet
- Acute Abdomen III: All Things UrologyDocument35 pagesAcute Abdomen III: All Things UrologyRumana IslamNo ratings yet
- WEAKER URINARY FLOW AND INCOMPLETE EMPTYINGDocument6 pagesWEAKER URINARY FLOW AND INCOMPLETE EMPTYINGFreddy PanjaitanNo ratings yet
- Vaginal Prolapse - Clinical PDFDocument83 pagesVaginal Prolapse - Clinical PDFanon_103011088No ratings yet
- UTI and Asymptomatic Bacteriuria TEACHING SLIDESDocument43 pagesUTI and Asymptomatic Bacteriuria TEACHING SLIDESJana DbaibouNo ratings yet
- What Is CircumcisionDocument4 pagesWhat Is Circumcisionelmore kakaNo ratings yet
- Workbook ActivityDocument2 pagesWorkbook ActivityRisciella 18No ratings yet
- General Questions About Sex: Frequently Asked Questions (Faqs)Document4 pagesGeneral Questions About Sex: Frequently Asked Questions (Faqs)Nitin DewanganNo ratings yet
- General SurgeryDocument83 pagesGeneral SurgeryCarlos HernándezNo ratings yet
- Female Condome How To UseDocument4 pagesFemale Condome How To UseRam Bahadur Saru100% (4)
- ExcretionDocument14 pagesExcretionAuthor ClubNo ratings yet
- Pyonefrosis Part 2Document8 pagesPyonefrosis Part 2Kevin MitnickNo ratings yet
- Surgery N Therapy List RGJYDocument57 pagesSurgery N Therapy List RGJYSandip PatilNo ratings yet
- STD Pre TestDocument2 pagesSTD Pre TestCrystal Ann Monsale TadiamonNo ratings yet
- 792Document527 pages792MarcNicaNo ratings yet
- DAFTAR PUSTAKA Referat Ruptur UretraDocument2 pagesDAFTAR PUSTAKA Referat Ruptur UretraDwi Ayu KusumawardaniNo ratings yet
- Pod Cast On Prevention of Catheter Associated Urinary Tract Infection 2Document12 pagesPod Cast On Prevention of Catheter Associated Urinary Tract Infection 2api-317345513No ratings yet
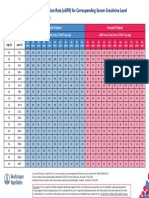
- Egfr ChartDocument1 pageEgfr ChartMahesh DoshiNo ratings yet
- Moderator: Mr. Ram Singh (Lecturer) Deptt. of Radio-Diagnosis & Imaging, PGIMER, ChandigarhDocument119 pagesModerator: Mr. Ram Singh (Lecturer) Deptt. of Radio-Diagnosis & Imaging, PGIMER, ChandigarhMunish DograNo ratings yet