You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Aortic AneurysmDocument61 pagesAortic AneurysmSurya Budikusuma64% (11)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
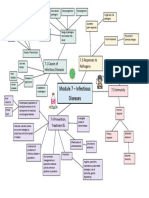
- Module 7 Mind Map BiologyDocument1 pageModule 7 Mind Map BiologyAltSpace TimeNo ratings yet
- 12 Bipolar & Mood DisordersDocument20 pages12 Bipolar & Mood DisordersSurya BudikusumaNo ratings yet
- Epidemiology of Cancers 2012Document52 pagesEpidemiology of Cancers 2012Surya Budikusuma100% (1)
- Malignant LymphomaDocument29 pagesMalignant LymphomaSurya BudikusumaNo ratings yet
- LeukopoiesisDocument30 pagesLeukopoiesisSurya Budikusuma100% (3)
- Hemoglobin MetabolismDocument80 pagesHemoglobin MetabolismSurya BudikusumaNo ratings yet
- Natural History of DiseaseDocument31 pagesNatural History of Diseasegabo dasNo ratings yet
- All Formulae BTR by DR Zainab VoraDocument18 pagesAll Formulae BTR by DR Zainab VoraRishabh MathurNo ratings yet
- Daftar Pustaka Aps OrangDocument3 pagesDaftar Pustaka Aps OrangAlexander DickyNo ratings yet
- Audit Program PpiDocument37 pagesAudit Program PpiIkrar DinataNo ratings yet
- The Final - Assignment Typhoid MaryDocument4 pagesThe Final - Assignment Typhoid Maryapi-311342690No ratings yet
- Pathogen Research AssignmentDocument2 pagesPathogen Research AssignmentDeven BaliNo ratings yet
- Emerging and Re Emerging DiseasesDocument63 pagesEmerging and Re Emerging DiseasesAljun MansalapusNo ratings yet
- 3.4 Cross-Sectional StudiesDocument4 pages3.4 Cross-Sectional StudiesRicardo Gomes100% (1)
- Measures of Association: by Fisaha.H (Bsc. Mphil)Document66 pagesMeasures of Association: by Fisaha.H (Bsc. Mphil)ruth100% (1)
- Bio Epidemiology Notes PDFDocument5 pagesBio Epidemiology Notes PDFEuni M.No ratings yet
- Disease Detectives NotesDocument4 pagesDisease Detectives NotesOwen LiuNo ratings yet
- A Study To Assess The Effectiveness of STP Regarding Knowledge of Preventive Measures On COPD Among Old Age People in Selected Village Rohtas BiharDocument6 pagesA Study To Assess The Effectiveness of STP Regarding Knowledge of Preventive Measures On COPD Among Old Age People in Selected Village Rohtas BiharIJARSCT Journal100% (1)
- Health Information Management of A Strategic Resource 4th Edition Abdelhak Test BankDocument8 pagesHealth Information Management of A Strategic Resource 4th Edition Abdelhak Test Bankoglepogy5kobgk100% (32)
- HES 007 2nd Periodical Exam TG Day 17Document3 pagesHES 007 2nd Periodical Exam TG Day 17AlbieRhioneilLatonioMacayanNo ratings yet
- Case Studies in Infectious Disease: Books and MediaDocument2 pagesCase Studies in Infectious Disease: Books and MediaherrerachaimNo ratings yet
- Lista DiagnosticeDocument566 pagesLista DiagnosticeGeanina MireaNo ratings yet
- Guideline Prevention of Communicable Diseases RCHD 1 Concepts of Communicable DiseasesDocument4 pagesGuideline Prevention of Communicable Diseases RCHD 1 Concepts of Communicable DiseasesGerald HanNo ratings yet
- Epidemiology Approach and MethodsDocument50 pagesEpidemiology Approach and MethodsBen PhiriNo ratings yet
- AOCase Control CohortstudydesignsDocument6 pagesAOCase Control CohortstudydesignsakshayajainaNo ratings yet
- Name of Student: Sta. Cruz National High School Health Declaration FormDocument1 pageName of Student: Sta. Cruz National High School Health Declaration FormRodney SajaNo ratings yet
- Measurements of Morbidity and MortalityDocument77 pagesMeasurements of Morbidity and MortalityAnasAbdelaNo ratings yet
- Toxicology - 2/03/16 What Is Epidemiology?Document3 pagesToxicology - 2/03/16 What Is Epidemiology?bella.marie.cunningham6770100% (1)
- Webinar Amal International Pedis Care FoundationDocument31 pagesWebinar Amal International Pedis Care Foundationdon rangerNo ratings yet
- c14 Microbiology Tortora TestbankDocument19 pagesc14 Microbiology Tortora Testbankwhitewave25No ratings yet
- Basic Measurements in EpidemiologyDocument24 pagesBasic Measurements in Epidemiologykrupa mathewNo ratings yet
- Accessory Adornment and Cross Infection in Direct Patient Care: A Literature ReviewDocument4 pagesAccessory Adornment and Cross Infection in Direct Patient Care: A Literature ReviewJoseph SquireNo ratings yet
- Bpharm Winter 2014Document1 pageBpharm Winter 2014babaf79912No ratings yet
- 23258-Article Text-66226-72029-10-20220731Document13 pages23258-Article Text-66226-72029-10-20220731Arifa LainaNo ratings yet
- Appraisal TherapyDocument3 pagesAppraisal TherapyDonniNo ratings yet