You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Guidelines For The Preparation of A Thesis at The Chair of Applied MicroeconomicsDocument6 pagesGuidelines For The Preparation of A Thesis at The Chair of Applied Microeconomicsformak_tejNo ratings yet
- Forbes and Lederman Class 4 ReferenceDocument20 pagesForbes and Lederman Class 4 Referenceformak_tejNo ratings yet
- GLMDocument12 pagesGLMformak_tejNo ratings yet
- Introduction To EconometricsDocument28 pagesIntroduction To Econometricsformak_tejNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ECON1203 HW Solution Week07Document5 pagesECON1203 HW Solution Week07Bad Boy0% (1)
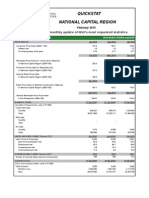
- Quickstat National Capital Region: A Monthly Update of NSO's Most Requested StatisticsDocument3 pagesQuickstat National Capital Region: A Monthly Update of NSO's Most Requested StatisticsDaniel John Cañares LegaspiNo ratings yet
- The History of Davao CityDocument12 pagesThe History of Davao CityLovely ClapisNo ratings yet
- Pio DuranDocument5 pagesPio DuranErold TarvinaNo ratings yet
- Applied Statistics enDocument282 pagesApplied Statistics enРадомир МутабџијаNo ratings yet
- Tutorial Sheet 2Document2 pagesTutorial Sheet 2Heman ChauhanNo ratings yet
- Multinomijalna RaspodelaDocument5 pagesMultinomijalna RaspodelaAbbé BusoniNo ratings yet
- Akan FinalDocument23 pagesAkan Finalanon_153131867100% (1)
- Bartlett-Arithmetic Growth PDFDocument29 pagesBartlett-Arithmetic Growth PDFSheena Mae Sietereales100% (1)
- 3201 Part B KasaragodDocument242 pages3201 Part B KasaragodKishore Thomas John ms17d020No ratings yet
- 01.a.demographic Projections - Aslam MahmoodDocument51 pages01.a.demographic Projections - Aslam MahmoodMaulikJoshiNo ratings yet
- Demography: Dr. Sheryl M. ReyesDocument18 pagesDemography: Dr. Sheryl M. ReyesNilda ReyesNo ratings yet
- Random Match Probability Worksheet, Version 0.5Document5 pagesRandom Match Probability Worksheet, Version 0.5sliterchewspensNo ratings yet
- CH03 ConfidenceIntervalEstimatesDocument11 pagesCH03 ConfidenceIntervalEstimatesutsav_koshtiNo ratings yet
- Workman & Niswander (1970)Document26 pagesWorkman & Niswander (1970)Mauricio MauricioNo ratings yet
- CMAP Census AnalysisDocument4 pagesCMAP Census AnalysisCrainsChicagoBusinessNo ratings yet
- Chapter 3 Final 1Document5 pagesChapter 3 Final 1Chanime Meih100% (1)
- Ch2 - Population ForecastingDocument5 pagesCh2 - Population Forecastingstaryklt0% (1)
- STA301 Solved MCQs With ReferenceDocument22 pagesSTA301 Solved MCQs With ReferenceAhsan Khan KhanNo ratings yet
- Statistics: Measure of Central Tendency MeanDocument25 pagesStatistics: Measure of Central Tendency MeanjlNo ratings yet
- Census of India, 2001Document31 pagesCensus of India, 2001K Prem RajNo ratings yet
- Mortpak ManualDocument78 pagesMortpak ManualAlfatihahRenoNo ratings yet
- Research Scaling & SamplingDocument66 pagesResearch Scaling & SamplingMukesh AgrawalNo ratings yet
- More Young Adults Are Living in Their ParentsDocument2 pagesMore Young Adults Are Living in Their ParentsTony AdamisNo ratings yet
- Questionnaire 4Document5 pagesQuestionnaire 4gregjefferson.cardinoNo ratings yet
- SummativeDocument2 pagesSummativeLourence DisoNo ratings yet
- Ethiopian Demography and Health: A Brief HistoryDocument9 pagesEthiopian Demography and Health: A Brief HistoryMillimoh AsfawNo ratings yet
- R-Lequin Graphic DescriptionDocument8 pagesR-Lequin Graphic DescriptionTyty AlxNo ratings yet
- Ekologi Populasi ItlDocument27 pagesEkologi Populasi ItlDwiMariaUlfahNo ratings yet
- Lecture6 Normal Probability Distribution PDFDocument6 pagesLecture6 Normal Probability Distribution PDFnauliNo ratings yet