You might also like
- Risk Factors & Prognosis For USMLE STEP 3 PDFDocument182 pagesRisk Factors & Prognosis For USMLE STEP 3 PDFSadia GhaniNo ratings yet
- Epidemiology of CVD DiseasesDocument19 pagesEpidemiology of CVD DiseaseshafizahhoshniNo ratings yet
- All About Ocean Life-Rachel BladonDocument6 pagesAll About Ocean Life-Rachel BladonRichard TekulaNo ratings yet
- Vendor Security ChecklistDocument11 pagesVendor Security ChecklistHarisNo ratings yet
- Resectoscopio 8677 Richard WolfDocument25 pagesResectoscopio 8677 Richard WolfManuel FloresNo ratings yet
- Cardiovascular Disease PreventionDocument17 pagesCardiovascular Disease Preventionchrissanto chandraNo ratings yet
- Coronary Artery DiseaseDocument80 pagesCoronary Artery Diseaseamelia pratiwiNo ratings yet
- PHN Assign 2Document13 pagesPHN Assign 2ghulam anooshaNo ratings yet
- Non-Communicable Disease Prevention and ControlDocument19 pagesNon-Communicable Disease Prevention and ControlJonnah Mae Belmonte100% (1)
- Cardiovascular Diseases (CVDS) : Key FactsDocument11 pagesCardiovascular Diseases (CVDS) : Key Factsriza kurniaNo ratings yet
- Risk Factors and Cardiovascular DiseaseDocument85 pagesRisk Factors and Cardiovascular DiseaseRachel LongoNo ratings yet
- DefiniciónDocument51 pagesDefiniciónKrissia SalvadorNo ratings yet
- Valensi Et Al, 2016.Document10 pagesValensi Et Al, 2016.Jeje MystearicaNo ratings yet
- Peripheral Vascular Disease - Wikipedia, The Free EncyclopediaDocument5 pagesPeripheral Vascular Disease - Wikipedia, The Free EncyclopediaDr. Mohammed AbdulWahab AlKhateebNo ratings yet
- Cardiometabolic Syndrome PipinDocument15 pagesCardiometabolic Syndrome Pipinspider_mechNo ratings yet
- Prasugrel and RosuvastatinDocument7 pagesPrasugrel and RosuvastatinMohammad Shahbaz AlamNo ratings yet
- Cardiovascular Disease (NCD) : o CORONARY HEART DISEASE (Ischemic Heart Disease)Document4 pagesCardiovascular Disease (NCD) : o CORONARY HEART DISEASE (Ischemic Heart Disease)Monica SabarreNo ratings yet
- Case Study CVDDocument8 pagesCase Study CVDChloe AguiNo ratings yet
- Epidemiology of Coronary Heart DiseasesDocument31 pagesEpidemiology of Coronary Heart DiseasesShaimaa EmadNo ratings yet
- Borja NV CDDocument4 pagesBorja NV CDKc Mea Paran BorjaNo ratings yet
- Managementul Pacientilor Boala Arteriala PerifericaDocument5 pagesManagementul Pacientilor Boala Arteriala PerifericaIrina NeamtuNo ratings yet
- FRC B. Cardiovascular Diseases OMS Key Facts and Questions.Document7 pagesFRC B. Cardiovascular Diseases OMS Key Facts and Questions.Eduardo AnayaNo ratings yet
- DHD - L5 - Heart Disease DiabetesDocument59 pagesDHD - L5 - Heart Disease Diabetesgp5d7nfjjpNo ratings yet
- Metabolic SyndromeDocument106 pagesMetabolic SyndromeLinda Hall Rothery100% (1)
- Cardiovascular Diseases - : Megan Phaul C. Kniazeff Mw2-1Document28 pagesCardiovascular Diseases - : Megan Phaul C. Kniazeff Mw2-1Kieth SeresulaNo ratings yet
- Cardiovascular Risk Factors in The Elderly: Baskent University Cardiology Dept., Ankara, TurkeyDocument23 pagesCardiovascular Risk Factors in The Elderly: Baskent University Cardiology Dept., Ankara, TurkeyMocanu Cristina-VioricaNo ratings yet
- Ischemic Heart DiseaseDocument47 pagesIschemic Heart DiseaseAbood SamoudiNo ratings yet
- Non Communicable DiseaseDocument9 pagesNon Communicable DiseasePulok HasanNo ratings yet
- Cardiovascular Diseases (CVDS) : Key FactsDocument5 pagesCardiovascular Diseases (CVDS) : Key FactsChantika ChikaNo ratings yet
- PAD Current InsightsDocument15 pagesPAD Current InsightsMaria PopNo ratings yet
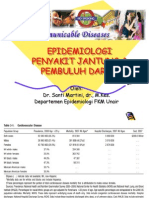
- Epidemiologi Penyakit Jantung & Pembuluh Darah: Oleh: Dr. Santi Martini, DR., M.Kes. Departemen Epidemiologi FKM UnairDocument42 pagesEpidemiologi Penyakit Jantung & Pembuluh Darah: Oleh: Dr. Santi Martini, DR., M.Kes. Departemen Epidemiologi FKM UnairareviamdNo ratings yet
- M4 Unit 1 Activity 2 Discussion NCM 112 LECDocument3 pagesM4 Unit 1 Activity 2 Discussion NCM 112 LECMaglangit, Lara MaeNo ratings yet
- CVDDocument25 pagesCVDSameer ValsangkarNo ratings yet
- 018 .Id - enDocument35 pages018 .Id - enAnonymous RN2t2v3No ratings yet
- Pattern of Stroke in Type 2 Diabetic Subjects Versus Non Diabetic SubjectsDocument4 pagesPattern of Stroke in Type 2 Diabetic Subjects Versus Non Diabetic SubjectsRobbi OcktadinataNo ratings yet
- J. Gonzales CDV BleedDocument3 pagesJ. Gonzales CDV BleedAra_Ongaco_8894No ratings yet
- PPISMP SEM 2 BIOLOGY Cardiovascular DiseaseDocument5 pagesPPISMP SEM 2 BIOLOGY Cardiovascular DiseaseMohamad Syafie Bin SamsirNo ratings yet
- Community Medicine Department Faculty of Medicine University of Indonesia Setyawati Budiningsih, Retno Asti Werdhani Nuri Purwito Adi April 4th 2012Document60 pagesCommunity Medicine Department Faculty of Medicine University of Indonesia Setyawati Budiningsih, Retno Asti Werdhani Nuri Purwito Adi April 4th 2012Faridah Yuwono 28No ratings yet
- Non Communicable Disease Prevention and ControlDocument36 pagesNon Communicable Disease Prevention and ControlElcid Pimentel100% (1)
- JournalDocument2 pagesJournalMichael FangkiNo ratings yet
- Peripheral Arterial Disease in People With Diabetes: Consensus StatementDocument9 pagesPeripheral Arterial Disease in People With Diabetes: Consensus StatementMoch Abdul RokimNo ratings yet
- Diabetes Complication LectureDocument63 pagesDiabetes Complication LectureDoni MarthenNo ratings yet
- Hypertension: Physiology, Pathophysiology and Clinical ManagementsDocument81 pagesHypertension: Physiology, Pathophysiology and Clinical ManagementsSonu SinghNo ratings yet
- Contemporaryandoptimal Medicalmanagementof PeripheralarterialdiseaseDocument18 pagesContemporaryandoptimal Medicalmanagementof PeripheralarterialdiseaseAnonymous kdBDppigENo ratings yet
- Management of Hypertension in Heart Failure: Matthew R. Jonovich and John D. BisognanoDocument15 pagesManagement of Hypertension in Heart Failure: Matthew R. Jonovich and John D. BisognanojagodicamiliNo ratings yet
- Toxins: Cardiotoxicity of Uremic Toxins: A Driver of Cardiorenal SyndromeDocument29 pagesToxins: Cardiotoxicity of Uremic Toxins: A Driver of Cardiorenal SyndromeIka AyuNo ratings yet
- Heart ProblemsDocument6 pagesHeart ProblemsLiang_Chun_5698No ratings yet
- Ksenija, MerokokDocument32 pagesKsenija, MerokokMUHAMMAD ILHAMNo ratings yet
- Diabetes: Nesreen Saadeh, MD Internal Medicine Department/ J.U.S.TDocument46 pagesDiabetes: Nesreen Saadeh, MD Internal Medicine Department/ J.U.S.TCWT2010No ratings yet
- Chief, Pediatric Medicine Valenzuela City Emergency HospitalDocument63 pagesChief, Pediatric Medicine Valenzuela City Emergency HospitalFevs BeeNo ratings yet
- Hypertension: Eu MBCHB 4 DR D M KillingoDocument73 pagesHypertension: Eu MBCHB 4 DR D M KillingoMalueth AnguiNo ratings yet
- Glycemic Control in Elderly Diabetes With Acute Coronary SyndromeDocument38 pagesGlycemic Control in Elderly Diabetes With Acute Coronary SyndromeWiwik Puji LestariNo ratings yet
- Coronary Artery DiseaseDocument6 pagesCoronary Artery DiseaseDivya PriyaNo ratings yet
- Diabetes and Stroke PreventionDocument11 pagesDiabetes and Stroke PreventionFarnida JamhalNo ratings yet
- Module 1 - Medical Background - Revised Oct 16Document38 pagesModule 1 - Medical Background - Revised Oct 16Wahyu WidiyantoNo ratings yet
- With A Healthy Heart, The Beat Goes On.Document4 pagesWith A Healthy Heart, The Beat Goes On.manish dafdaNo ratings yet
- Report From The Canadian Chronic Disease Surveillance System - Heart Disease in Canada, 2018 - Canada - CaDocument77 pagesReport From The Canadian Chronic Disease Surveillance System - Heart Disease in Canada, 2018 - Canada - CaRegina EnggelineNo ratings yet
- Myocardial InfarctionDocument21 pagesMyocardial Infarctionanon_516349434No ratings yet
- Enfermedad Arterial Coronaria en Pacientes DiabéticosDocument10 pagesEnfermedad Arterial Coronaria en Pacientes DiabéticosmacrisgabelaNo ratings yet
- Unveiling the Unseen: A Journey Into the Hearts Labyrinth SeanFrom EverandUnveiling the Unseen: A Journey Into the Hearts Labyrinth SeanNo ratings yet
- Curs4 Tradus EnglezaDocument64 pagesCurs4 Tradus EnglezaArina ChifulescuNo ratings yet
- Fertility Preservation: UMF "Carol Davila" - Embryology Department, Anatomy DisciplineDocument53 pagesFertility Preservation: UMF "Carol Davila" - Embryology Department, Anatomy DisciplineArina ChifulescuNo ratings yet
- Fertility Preservation: UMF "Carol Davila" - Embryology Department, Anatomy DisciplineDocument53 pagesFertility Preservation: UMF "Carol Davila" - Embryology Department, Anatomy DisciplineArina ChifulescuNo ratings yet
- Techniques For Assisted Human ReproductionDocument51 pagesTechniques For Assisted Human ReproductionArina ChifulescuNo ratings yet
- Curs2 Tradus EnglezaDocument75 pagesCurs2 Tradus EnglezaArina ChifulescuNo ratings yet
- Techniques For Assisted Human ReproductionDocument51 pagesTechniques For Assisted Human ReproductionArina ChifulescuNo ratings yet
- Paclitaxel Against Cancer A Short Review 2161 0444.1000130Document3 pagesPaclitaxel Against Cancer A Short Review 2161 0444.1000130Arina ChifulescuNo ratings yet
- Operativeobstetrics 121102075034 Phpapp01Document32 pagesOperativeobstetrics 121102075034 Phpapp01Arina Chifulescu100% (1)
- Curs1 Tradus EnglezaDocument58 pagesCurs1 Tradus EnglezaArina ChifulescuNo ratings yet
- Teste PsihiatrieDocument22 pagesTeste PsihiatrieArina ChifulescuNo ratings yet
- Curs 2012 Monitoring in AnesthesiaDocument105 pagesCurs 2012 Monitoring in AnesthesiaCarmen DuranNo ratings yet
- Anti Bio Gram ADocument38 pagesAnti Bio Gram ADenisa OprisanescuNo ratings yet
- Diselectrolitemii 2015novDocument106 pagesDiselectrolitemii 2015novArina ChifulescuNo ratings yet
- Diabetic Macrovascular DiseaseDocument31 pagesDiabetic Macrovascular DiseaseArina ChifulescuNo ratings yet
- Application of Different Fruit Peels FormulationsDocument3 pagesApplication of Different Fruit Peels FormulationsYvette GarciaNo ratings yet
- Pediatric Medication Dosing GuildelinesDocument2 pagesPediatric Medication Dosing GuildelinesMuhammad ZeeshanNo ratings yet
- Knopp2017 Article OnceACheaterAlwaysACheaterSeriDocument11 pagesKnopp2017 Article OnceACheaterAlwaysACheaterSeriAnda F. CotoarăNo ratings yet
- Fishing Broken Wire: WCP Slickline Europe Learning Centre SchlumbergerDocument23 pagesFishing Broken Wire: WCP Slickline Europe Learning Centre SchlumbergerAli AliNo ratings yet
- Form Apr 22 2022Document4 pagesForm Apr 22 2022api-589628245No ratings yet
- Profometer 5brochureDocument2 pagesProfometer 5brochureLKBB Fakultas TeknikNo ratings yet
- OSCE Pediatric Dentistry Lecture-AnswersDocument40 pagesOSCE Pediatric Dentistry Lecture-AnswersR MNo ratings yet
- Clack 2983 WS1EE Twin Valve LDocument2 pagesClack 2983 WS1EE Twin Valve Lmohamed boufasNo ratings yet
- Trash Chute-Compliance Sheet Sangir)Document5 pagesTrash Chute-Compliance Sheet Sangir)Li LiuNo ratings yet
- of Biology On Introductory BioinformaticsDocument13 pagesof Biology On Introductory BioinformaticsUttkarsh SharmaNo ratings yet
- TinyEYE Online Speech Therapy Media GuideDocument4 pagesTinyEYE Online Speech Therapy Media GuideTinyEYE Therapy ServicesNo ratings yet
- People v. Jerry BugnaDocument1 pagePeople v. Jerry BugnaRey Malvin SG PallominaNo ratings yet
- Hemorrhagic Shock (Anestesi)Document44 pagesHemorrhagic Shock (Anestesi)Dwi Meutia IndriatiNo ratings yet
- APPLE FRITTER CAKE Cook Heavenly RecipesDocument4 pagesAPPLE FRITTER CAKE Cook Heavenly Recipes1940LaSalleNo ratings yet
- Seed PrimingDocument4 pagesSeed PrimingbigbangNo ratings yet
- Female Education ThesisDocument48 pagesFemale Education ThesisHashmie Ali73% (11)
- Trust His Heart: - J - J J - . JDocument10 pagesTrust His Heart: - J - J J - . JJa-Cy R4o15se04roNo ratings yet
- Clay Analysis - 1Document55 pagesClay Analysis - 1JCSNo ratings yet
- Significant Supreme Court RulingsDocument5 pagesSignificant Supreme Court Rulingsapi-307941674No ratings yet
- iGCSE Biology Section 1 Lesson 1Document44 pagesiGCSE Biology Section 1 Lesson 1aastha dograNo ratings yet
- Indian MaDocument1 pageIndian MaAnass LyamaniNo ratings yet
- Jan Precious Mille BDocument1 pageJan Precious Mille BJebjeb C. BrañaNo ratings yet
- Location: Map of Naga CityDocument2 pagesLocation: Map of Naga Citycatherine boragayNo ratings yet
- Physical Fitness TestDocument1 pagePhysical Fitness TestGiessen Fran RamosNo ratings yet
- Ball Bearing Units Stainless SeriesDocument5 pagesBall Bearing Units Stainless SeriesRicardo KharisNo ratings yet
- Patanjali CHP 1Document31 pagesPatanjali CHP 1Prasad KadamNo ratings yet
- Recipe Booklet PRINT VERSIONDocument40 pagesRecipe Booklet PRINT VERSIONjtsunami815100% (1)