You might also like
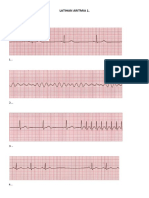
- Latihan Aritmia 1.: Bacalah ECG Di Bawah IniDocument8 pagesLatihan Aritmia 1.: Bacalah ECG Di Bawah Inianggarayudha89No ratings yet
- Epilepsi Bangkitan Umum Tonik-Klonik Di UGD RSUP Sanglah Denpasar-BaliDocument5 pagesEpilepsi Bangkitan Umum Tonik-Klonik Di UGD RSUP Sanglah Denpasar-BaliZakia DrajatNo ratings yet
- CamScanner App Scans Documents EasilyDocument2 pagesCamScanner App Scans Documents Easilyanggarayudha89No ratings yet
- Rome III Diagnostic Criteria FGIDsDocument14 pagesRome III Diagnostic Criteria FGIDsPutu Reza Sandhya PratamaNo ratings yet
- Adverse Reaction To FoodsDocument28 pagesAdverse Reaction To Foodsanggarayudha89No ratings yet
- Simpsons Forensic Page 67-68Document3 pagesSimpsons Forensic Page 67-68anggarayudha89No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Patent EsDocument10 pagesPatent Esalcorrea2009No ratings yet
- Konsep Dasar ToksikologiDocument63 pagesKonsep Dasar ToksikologiSaber LohengarmNo ratings yet
- (Dorothy Nelkin, M. Susan Lindee) The DNA MystiqueDocument314 pages(Dorothy Nelkin, M. Susan Lindee) The DNA MystiqueAntonella ParisiNo ratings yet
- Entamoeba histolytica (True PathogenDocument112 pagesEntamoeba histolytica (True PathogenMiaQuiambaoNo ratings yet
- Gene Mapping AssignmentDocument6 pagesGene Mapping AssignmentJay MenonNo ratings yet
- UGSemsterSyllabus Zoology 6Sem8A619Zoology English SilkWarmbreeding PDFDocument95 pagesUGSemsterSyllabus Zoology 6Sem8A619Zoology English SilkWarmbreeding PDFhidara71580% (1)
- Asmi 03 0500Document3 pagesAsmi 03 0500Trapti JadonNo ratings yet
- NBSAP Canada EngDocument91 pagesNBSAP Canada Eng王也No ratings yet
- Starch and Microbial α-Amylases: From Concepts to Biotechnological ApplicationsDocument30 pagesStarch and Microbial α-Amylases: From Concepts to Biotechnological ApplicationsIndrayana PratamaNo ratings yet
- OCR A A-Level Biology Retrieval Roulette COMPLETEDocument115 pagesOCR A A-Level Biology Retrieval Roulette COMPLETEtikif31811No ratings yet
- Department of Education: Tle-Cookery Assessment - Grade 10 Quarter 1 Week 1Document2 pagesDepartment of Education: Tle-Cookery Assessment - Grade 10 Quarter 1 Week 1IvyRoseBarcilloAlivioNo ratings yet
- Lesson1: Cell, The Basic Unit of LifeDocument4 pagesLesson1: Cell, The Basic Unit of Lifedream kingNo ratings yet
- Immunoglobulins ClassDocument16 pagesImmunoglobulins ClassKoushali BanerjeeNo ratings yet
- PROTOZOA DARAH (MALARIADocument88 pagesPROTOZOA DARAH (MALARIAGladis Aprilla RizkiNo ratings yet
- Ginther, 1998 Equine PregnancyDocument32 pagesGinther, 1998 Equine PregnancyAdrian Ayala GutierrezNo ratings yet
- Advanced Cell BiologyDocument14 pagesAdvanced Cell BiologyUmair AneesNo ratings yet
- Kanamycin Summary Report 2 Committee Veterinary Medicinal Products - enDocument9 pagesKanamycin Summary Report 2 Committee Veterinary Medicinal Products - enilhamNo ratings yet
- Alpha CRS+: Cellular Vitality ComplexDocument5 pagesAlpha CRS+: Cellular Vitality ComplexRam TamangNo ratings yet
- Sophia Human Biology Lab SyllabusDocument6 pagesSophia Human Biology Lab SyllabusKoffi Agbéko HonsouNo ratings yet
- 1730 3631 1 PBDocument10 pages1730 3631 1 PB19-2024 Ananda Hera UtamaNo ratings yet
- Food Chain SimulationDocument5 pagesFood Chain SimulationJose CabezasNo ratings yet
- Cell JunctionDocument63 pagesCell JunctionsphuyalNo ratings yet
- Pharmacology NotesDocument4 pagesPharmacology NotesKristoffer VelezNo ratings yet
- Chapter 03Document4 pagesChapter 03Teehee JonesNo ratings yet
- Phytochemical and Antibacterial Screening of Andropogon aciculatusDocument38 pagesPhytochemical and Antibacterial Screening of Andropogon aciculatusKemtOot Ruizo100% (1)
- BIOENG - FA1-2 (Combined)Document21 pagesBIOENG - FA1-2 (Combined)Aceriel VillanuevaNo ratings yet
- Cladogram CH 19 Part ADocument3 pagesCladogram CH 19 Part AJasmine lee100% (1)
- 5 Fotosintesi 2 PDFDocument99 pages5 Fotosintesi 2 PDFLuca DelvecchioNo ratings yet
- Cell Biology Product and Research Guide PDFDocument164 pagesCell Biology Product and Research Guide PDFBasma Al-KershNo ratings yet
- Secondary Structure of ProteinDocument3 pagesSecondary Structure of ProteinSahrEmmanuelJr.No ratings yet