You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 87EOLT49DDocument6 pages87EOLT49DGlecy AdrianoNo ratings yet
- Circulatory System - Arterial & Venous TreesDocument28 pagesCirculatory System - Arterial & Venous TreesItharshan IndreswaranNo ratings yet
- SVTDocument8 pagesSVTJulieNo ratings yet
- The Complete Guide To Vascular Ultrasound PDFDocument146 pagesThe Complete Guide To Vascular Ultrasound PDFAnna Sofía ParedesNo ratings yet
- Final Announcement REV 5 200523Document24 pagesFinal Announcement REV 5 200523AgilSugiaNo ratings yet
- Blood Supply of Brain and Spinal CordDocument32 pagesBlood Supply of Brain and Spinal CordShalini SinghNo ratings yet
- #7assess CV Function Physical ExamDocument27 pages#7assess CV Function Physical Examkimberly dedaseNo ratings yet
- Full Paper Template ICoHS 2021 NormaliyantiDocument12 pagesFull Paper Template ICoHS 2021 NormaliyantiMade Adhitya AffandaNo ratings yet
- Transport in Humans: 8.1 Need For Transport SystemDocument11 pagesTransport in Humans: 8.1 Need For Transport Systemka klklklNo ratings yet
- Vascular Laboratory Arterial RuthefordDocument17 pagesVascular Laboratory Arterial RuthefordRosanyi JimenezNo ratings yet
- AHA Examination Auscultation Part IVDocument42 pagesAHA Examination Auscultation Part IVHananya ManroeNo ratings yet
- Linfedema: Actualización en El Diagnóstico y Tratamiento QuirúrgicoDocument10 pagesLinfedema: Actualización en El Diagnóstico y Tratamiento QuirúrgicoHumberto Salas VelizNo ratings yet
- An Assignment On Surgery subject:-SHOCK (Definition, Classification and Pathophysiology of Shock)Document8 pagesAn Assignment On Surgery subject:-SHOCK (Definition, Classification and Pathophysiology of Shock)manish soniNo ratings yet
- LITFL - Wellens SyndromeDocument8 pagesLITFL - Wellens Syndromesunil abrahamNo ratings yet
- CVK Kod Djece, DužinaDocument4 pagesCVK Kod Djece, DužinaDamir PištoljevićNo ratings yet
- Updates On Pulmonary HypertensionDocument39 pagesUpdates On Pulmonary HypertensionZurlin DwirostantinNo ratings yet
- Basic Science Anaesthesia Update 2008Document200 pagesBasic Science Anaesthesia Update 2008Ruben Kovač100% (1)
- Athlete's Heart: Dr. Arzalan BaigDocument59 pagesAthlete's Heart: Dr. Arzalan BaigArzalan BaigNo ratings yet
- Icn Lec TransDocument43 pagesIcn Lec TransHannah DuyagNo ratings yet
- Chronic Heart Failure in Congenital Heart Disease: AHA Scientific StatementDocument33 pagesChronic Heart Failure in Congenital Heart Disease: AHA Scientific StatementLufthi FahrezaNo ratings yet
- Lesson-Proper of A Lesson PlanDocument2 pagesLesson-Proper of A Lesson PlanNhicolle DancelNo ratings yet
- Sherif Mokhtar, MD: Professor of Cardiology, Professor of Critical Care Medicine Cairo UniversityDocument85 pagesSherif Mokhtar, MD: Professor of Cardiology, Professor of Critical Care Medicine Cairo UniversityShimmering MoonNo ratings yet
- Drugs Acting On Cardio Vascular SystemDocument16 pagesDrugs Acting On Cardio Vascular SystemANUSHYA B PSGRKCWNo ratings yet
- Thorax Multiple Choice Questions AnswersDocument27 pagesThorax Multiple Choice Questions AnswersNick Jacob88% (25)
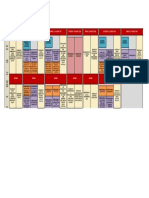
- Program at Glance WECOC 2021-Updated Juli 2021Document1 pageProgram at Glance WECOC 2021-Updated Juli 2021Bambang SupriadiNo ratings yet
- Brugia MalayiDocument4 pagesBrugia MalayiJericha IsidroNo ratings yet
- Acynotic Congenital Heart Diseases: FFU May 2020Document14 pagesAcynotic Congenital Heart Diseases: FFU May 2020gibreilNo ratings yet
- Stroke Topic DiscussionDocument19 pagesStroke Topic Discussionapi-648714317No ratings yet
- Basic Objectives of Color and Spectral DopplerDocument5 pagesBasic Objectives of Color and Spectral DopplerAsaad Baloch100% (2)
- Renal VeinDocument18 pagesRenal VeinAbhi KumarNo ratings yet