You might also like
- 9 Vital SignsDocument103 pages9 Vital Signsasnake DagnewNo ratings yet
- Nursing Basics Vital SignsDocument22 pagesNursing Basics Vital SignsTee WoodNo ratings yet
- Empyema 171013100219Document23 pagesEmpyema 171013100219Mahmoud Abdel MoneimNo ratings yet
- Bedbath & Perineal CareDocument22 pagesBedbath & Perineal CarealelichengNo ratings yet
- Concept of Handwashing Ncma113 LabDocument4 pagesConcept of Handwashing Ncma113 Labeverly evangelistaNo ratings yet
- Vital SignsDocument74 pagesVital SignsSofyan Hadi Saputra100% (1)
- Nursing Care of Patients With Cardiac ProblemsDocument125 pagesNursing Care of Patients With Cardiac ProblemsAyeNo ratings yet
- Which of The Following Statements by The Nurse WouldDocument7 pagesWhich of The Following Statements by The Nurse WouldFreeNursingNotesNo ratings yet
- Prepared by Mary Ann A. Cubon, RN, RM, ManDocument35 pagesPrepared by Mary Ann A. Cubon, RN, RM, ManCarlaLuisaVillalunaNo ratings yet
- Unit 1: Introduction: The Nursing ProcessDocument7 pagesUnit 1: Introduction: The Nursing ProcessMeyden PringNo ratings yet
- Promoting Safety in Healthcare EnvDocument13 pagesPromoting Safety in Healthcare EnvnamNo ratings yet
- Understanding Fever: Causes, Types, and Nursing CareDocument21 pagesUnderstanding Fever: Causes, Types, and Nursing CareTele NursingNo ratings yet
- Seminar On Venilator CareDocument15 pagesSeminar On Venilator CareISLAMIC KNOWLEDGE BASED ON TRULY HADISNo ratings yet
- Promoting Personal Hygiene & Promoting Rest & SleepDocument26 pagesPromoting Personal Hygiene & Promoting Rest & SleepYousef JafarNo ratings yet
- Burns Practice TeachingDocument58 pagesBurns Practice TeachingSakthi Devi100% (1)
- Physical Examination 2003Document39 pagesPhysical Examination 2003Gayatri MudliyarNo ratings yet
- CVP MonitoringDocument24 pagesCVP MonitoringChoji Heiwajima100% (1)
- Oxygen InhalationDocument44 pagesOxygen InhalationDr. Jayesh Patidar67% (3)
- Unit 6 Hot and Cold ApplicationDocument9 pagesUnit 6 Hot and Cold ApplicationElaine Frances IlloNo ratings yet
- Management of Asthma ExacerbationDocument13 pagesManagement of Asthma ExacerbationAini Shofa HaniahNo ratings yet
- Tepid Sponge/Cold SpongeDocument2 pagesTepid Sponge/Cold SpongeCheryl PorpayasNo ratings yet
- Nursing and End-of-Life CareDocument26 pagesNursing and End-of-Life CareShafiq Ur RahmanNo ratings yet
- Lecturer/ Magda Bayoumi: Prepared byDocument22 pagesLecturer/ Magda Bayoumi: Prepared byicrs_aamirNo ratings yet
- Approach To An Unconscious Patient-OyeyemiDocument41 pagesApproach To An Unconscious Patient-OyeyemiOyeyemi AdeyanjuNo ratings yet
- Management of Clients With Burns and ShockDocument7 pagesManagement of Clients With Burns and ShockJunah Marie Rubinos Palarca0% (1)
- Rheumatic Heart DiseaseDocument10 pagesRheumatic Heart DiseaseSuhas IngaleNo ratings yet
- Main Applications of ECG DiagnosisDocument19 pagesMain Applications of ECG DiagnosisMaria Rowena O. SalvoNo ratings yet
- Vital Signs: Pulse & Blood PressureDocument47 pagesVital Signs: Pulse & Blood Pressurenessa100% (1)
- UTI Guide: Symptoms, Causes & TreatmentDocument39 pagesUTI Guide: Symptoms, Causes & TreatmentSabita TripathiNo ratings yet
- Patient Rights & Organizational EthicsDocument17 pagesPatient Rights & Organizational EthicsBOnn EljayNo ratings yet
- English Recovery RoomDocument5 pagesEnglish Recovery RoomRahima PutriNo ratings yet
- Ostomy Care: Esther Hattler, BS, RN, WCCDocument51 pagesOstomy Care: Esther Hattler, BS, RN, WCCAnita TermasNo ratings yet
- Bed Bath MikeDocument24 pagesBed Bath MikeMike100% (1)
- Introduction To Medical Surgical NursingDocument42 pagesIntroduction To Medical Surgical NursingAmanuel MaruNo ratings yet
- Treadmill Test: Khairul Nizam Abdul Rahman 4262143008Document12 pagesTreadmill Test: Khairul Nizam Abdul Rahman 4262143008Dea Amelia YolandaNo ratings yet
- Patient SafetyDocument18 pagesPatient SafetySuhatman AhNo ratings yet
- SEIZURE DISORDER: CAUSES, TYPES, SIGNS AND TREATMENTDocument70 pagesSEIZURE DISORDER: CAUSES, TYPES, SIGNS AND TREATMENTRohini RaiNo ratings yet
- Physiology of Hearing: Departemen Fisiologi FK UsuDocument28 pagesPhysiology of Hearing: Departemen Fisiologi FK UsuSonia P SNo ratings yet
- Thromboangiitis Obliterans (Buerger Disease)Document12 pagesThromboangiitis Obliterans (Buerger Disease)Sheila AzelyaNo ratings yet
- Nurse Objective Type QuestionsDocument36 pagesNurse Objective Type QuestionsGnanaprakasam AntonyNo ratings yet
- Admission & Discharge FONDocument43 pagesAdmission & Discharge FONMedicoholic Dr.No ratings yet
- Asthma (Reactive Airway Disease)Document33 pagesAsthma (Reactive Airway Disease)anwar jabariNo ratings yet
- Admission and EmergencyDocument12 pagesAdmission and EmergencyRashid AyubiNo ratings yet
- What Is ICU PsychosisDocument6 pagesWhat Is ICU PsychosisAngelicaMarieRafananNo ratings yet
- Airway SuctioningDocument30 pagesAirway SuctioningPearl DiBerardinoNo ratings yet
- Checklists of Respiratory System AssessmentDocument22 pagesChecklists of Respiratory System AssessmentDhrumini PatelNo ratings yet
- Chest Injuries GuideDocument19 pagesChest Injuries GuideAbdi Kumala100% (1)
- Nursing management of peritoneal dialysis patientsDocument27 pagesNursing management of peritoneal dialysis patientsHemantNo ratings yet
- Nursing Care of Clients Before and After CABGDocument46 pagesNursing Care of Clients Before and After CABGshejila c hNo ratings yet
- Immediate Care of NewbornDocument4 pagesImmediate Care of NewbornjvjohnNo ratings yet
- Blood TransfusionDocument5 pagesBlood TransfusionMoustafa Hazzaa100% (1)
- Gowning, Gloving (Open and Closed Techniques-Unassisted)Document11 pagesGowning, Gloving (Open and Closed Techniques-Unassisted)Grape JuiceNo ratings yet
- Umbilical Artery Catheterization for Blood Pressure MonitoringDocument11 pagesUmbilical Artery Catheterization for Blood Pressure MonitoringRhaq Sheldon-CoelhoNo ratings yet
- Bed Making: Prepared By:-Lemesa ADocument34 pagesBed Making: Prepared By:-Lemesa ASori Kasasa0% (1)
- Infection and Infectious ProcessDocument44 pagesInfection and Infectious Processpandey omkarNo ratings yet
- Exercise vs Immobility EffectsDocument110 pagesExercise vs Immobility EffectsAshaNo ratings yet
- Burns MGNT and CalculationDocument7 pagesBurns MGNT and CalculationPoova RagavanNo ratings yet
- Disseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDisseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pemeriksaan Tanda Vital-Kuliah PengantarDocument22 pagesPemeriksaan Tanda Vital-Kuliah PengantarDwitia IswariNo ratings yet
- Landero Clinic and Hospital: Notice of ChargeDocument1 pageLandero Clinic and Hospital: Notice of ChargeQuennie Marie Moreno VillanuevaNo ratings yet
- VL SupeDocument1 pageVL SupeQuennie Marie Moreno VillanuevaNo ratings yet
- Nursing Code Blue PolicyDocument13 pagesNursing Code Blue PolicyQuennie Marie Moreno VillanuevaNo ratings yet
- UPHSD-LP College of Nursing (AHSE-2A Batch 2007-2008)Document1 pageUPHSD-LP College of Nursing (AHSE-2A Batch 2007-2008)Quennie Marie Moreno VillanuevaNo ratings yet
- Bedroom NegotiationsDocument344 pagesBedroom NegotiationsAnonymous 0CCpB9Z61% (18)
- Alphabetizing and RhymingDocument13 pagesAlphabetizing and RhymingQuennie Marie Moreno VillanuevaNo ratings yet
- E.O. 51 and RIRRDocument29 pagesE.O. 51 and RIRRcorzpun168678100% (6)
- ReferencesDocument3 pagesReferencesQuennie Marie Moreno VillanuevaNo ratings yet
- 2012 WHD AgeingDocument4 pages2012 WHD AgeingQuennie Marie Moreno VillanuevaNo ratings yet
- Childrearing Practices MothersDocument4 pagesChildrearing Practices MothersQuennie Marie Moreno VillanuevaNo ratings yet
- 10 Steps To Successful Breastfeeding 2Document39 pages10 Steps To Successful Breastfeeding 2Quennie Marie Moreno VillanuevaNo ratings yet
- Dengue Fever FactsDocument12 pagesDengue Fever FactsQuennie Marie Moreno VillanuevaNo ratings yet
- Attendance Sheet BreastfeedingDocument1 pageAttendance Sheet BreastfeedingQuennie Marie Moreno VillanuevaNo ratings yet
- Child Rearing Practices Vary by CultureDocument2 pagesChild Rearing Practices Vary by CultureQuennie Marie Moreno VillanuevaNo ratings yet
- Early Childhood CariesDocument69 pagesEarly Childhood CariesQuennie Marie Moreno VillanuevaNo ratings yet
- 10 Myths About SchizophreniaDocument11 pages10 Myths About SchizophreniaQuennie Marie Moreno VillanuevaNo ratings yet
- An Educational Learning Module To Enhance Communication SkillsDocument39 pagesAn Educational Learning Module To Enhance Communication SkillsQuennie Marie Moreno VillanuevaNo ratings yet
- JournalDocument12 pagesJournalQuennie Marie Moreno VillanuevaNo ratings yet
- Childgçös RightsDocument57 pagesChildgçös RightsQuennie Marie Moreno VillanuevaNo ratings yet
- Chapter 2 Electronic StructureDocument62 pagesChapter 2 Electronic StructureLivan TuahNo ratings yet
- 6.water Treatment and Make-Up Water SystemDocument18 pages6.water Treatment and Make-Up Water Systempepenapao1217100% (1)
- Kloos Community Psychology Book FlyerDocument2 pagesKloos Community Psychology Book FlyerRiska MirantiNo ratings yet
- Understanding Empathy and SympathyDocument2 pagesUnderstanding Empathy and SympathyFrinces MarvidaNo ratings yet
- H1 Revision Notes DNA and GenomicsDocument6 pagesH1 Revision Notes DNA and GenomicsJiaLi XieNo ratings yet
- Ulcus Decubitus PDFDocument9 pagesUlcus Decubitus PDFIrvan FathurohmanNo ratings yet
- Rise School of Accountancy Test 08Document5 pagesRise School of Accountancy Test 08iamneonkingNo ratings yet
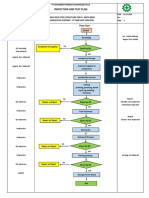
- Inspection and Test Plan: Flow Chart Start IncomingDocument1 pageInspection and Test Plan: Flow Chart Start IncomingSinden AyuNo ratings yet
- PR Cuisine vs US CuisineDocument2 pagesPR Cuisine vs US CuisineJannette HernandezNo ratings yet
- Vietnam Snack Market Grade BDocument3 pagesVietnam Snack Market Grade BHuỳnh Điệp TrầnNo ratings yet
- Density of Aggregates: ObjectivesDocument4 pagesDensity of Aggregates: ObjectivesKit Gerald EliasNo ratings yet
- Darnell's Father Goes StrictDocument2 pagesDarnell's Father Goes StrictDavid Theodore Richardson IIINo ratings yet
- Build Size and Aesthetics with the 6-Week Hype Gains Hypertrophy ProgramDocument21 pagesBuild Size and Aesthetics with the 6-Week Hype Gains Hypertrophy ProgramDanCurtis100% (1)
- Ethnobotany Manual 14th September 2016Document54 pagesEthnobotany Manual 14th September 2016Rahul0% (1)
- Genset Ops Manual 69ug15 PDFDocument51 pagesGenset Ops Manual 69ug15 PDFAnonymous NYymdHgy100% (1)
- CHAPTER 15 Managing Current AssetsDocument26 pagesCHAPTER 15 Managing Current AssetsAhsanNo ratings yet
- Rundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967Document15 pagesRundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967nixyingboNo ratings yet
- Methodology For The Validation of Fuel Consumption in Diesel Engines Installed On Board Military Ships, Using Diesel Oil and Biodiesel BlendsDocument16 pagesMethodology For The Validation of Fuel Consumption in Diesel Engines Installed On Board Military Ships, Using Diesel Oil and Biodiesel BlendsErick RodriguesNo ratings yet
- Human Resources Management Article Review On "The 3 Essential Jobs That Most Retention Programs Ignore"Document14 pagesHuman Resources Management Article Review On "The 3 Essential Jobs That Most Retention Programs Ignore"Pang Kok ShengNo ratings yet
- SBI - Certificate To Be Submitted by Pensioner - ChandigarhDocument1 pageSBI - Certificate To Be Submitted by Pensioner - ChandigarhMsinghNo ratings yet
- Flexible and Alternative Seating: in ClassroomsDocument5 pagesFlexible and Alternative Seating: in ClassroomsweningNo ratings yet
- Small Gas Turbines 4 LubricationDocument19 pagesSmall Gas Turbines 4 LubricationValBMSNo ratings yet
- The Motive Journal (3rd Edition)Document42 pagesThe Motive Journal (3rd Edition)Shubham Sharma0% (1)
- Introduction To Integrative Homeopathy - Bob LeckridgeDocument16 pagesIntroduction To Integrative Homeopathy - Bob LeckridgeBob LeckridgeNo ratings yet
- HBSE-Mock ExamDocument3 pagesHBSE-Mock ExamAnneNo ratings yet
- Overhead Set (OBC)Document19 pagesOverhead Set (OBC)MohamedNo ratings yet
- Environmental Product Declaration: PU EuropeDocument6 pagesEnvironmental Product Declaration: PU EuropeIngeniero Mac DonnellNo ratings yet
- 0001 CatDocument108 pages0001 CatJorge CabreraNo ratings yet
- CASR Part 830 Amdt. 2 - Notification & Reporting of Aircraft Accidents, Incidents, or Overdue Acft & Investigation OCRDocument17 pagesCASR Part 830 Amdt. 2 - Notification & Reporting of Aircraft Accidents, Incidents, or Overdue Acft & Investigation OCRHarry NuryantoNo ratings yet
- Causes of DyspneaDocument9 pagesCauses of DyspneaHanis Afiqah Violet MeowNo ratings yet