You might also like
- Mechanisms of Antibiotic Resistance in BacteriaDocument41 pagesMechanisms of Antibiotic Resistance in BacteriajaneNo ratings yet
- Antibiotics – Are They Curing Us or Killing Us?: The Catastrophic Impact of the Over-prescription of Antibiotics on Our HealthFrom EverandAntibiotics – Are They Curing Us or Killing Us?: The Catastrophic Impact of the Over-prescription of Antibiotics on Our HealthNo ratings yet
- Antibiotics, Misuse and ConsequencesDocument67 pagesAntibiotics, Misuse and Consequencestummalapalli venkateswara raoNo ratings yet
- 8 - Microbes and DiseaseDocument6 pages8 - Microbes and DiseaseHarry DouglasNo ratings yet
- Antibiotic Resistance and The Susceptibility of Bacteria LabDocument19 pagesAntibiotic Resistance and The Susceptibility of Bacteria LabsciencystuffNo ratings yet
- Presentation On Antibiotic: By:-Shiv Kumar Roll No. 21 Mba BTDocument18 pagesPresentation On Antibiotic: By:-Shiv Kumar Roll No. 21 Mba BTAnshuman ParasharNo ratings yet
- Study Drug Resistance in Bacteria Using AntibioticsDocument47 pagesStudy Drug Resistance in Bacteria Using Antibioticskioilui;lphio961% (18)
- Bacterial ResistanceDocument9 pagesBacterial ResistanceShifa RazaNo ratings yet
- Antibiotics: Success and FailuresDocument43 pagesAntibiotics: Success and Failurestummalapalli venkateswara raoNo ratings yet
- Antibiotic Resistance in BacteriaDocument14 pagesAntibiotic Resistance in BacteriaIrfa NadeemNo ratings yet
- Martens and Demain - , 2017 - The AntibiotiDocument7 pagesMartens and Demain - , 2017 - The AntibiotiJavier CastroNo ratings yet
- Biology Project XiiDocument14 pagesBiology Project XiiSagayaraniNo ratings yet
- Projan - Antibiotics Where Now 2008Document56 pagesProjan - Antibiotics Where Now 2008Vincent GeruszNo ratings yet
- Antibiotic Resistance: Audience-Senior Medical Officers Venue-Pune Date - 9 May 2011Document42 pagesAntibiotic Resistance: Audience-Senior Medical Officers Venue-Pune Date - 9 May 2011J NuchinNo ratings yet
- Mekanisme Resistensi Antibiotik - 2014Document10 pagesMekanisme Resistensi Antibiotik - 2014ArdieNo ratings yet
- Antimicrobial Resistances: The World's Next Pandemic On The WayDocument11 pagesAntimicrobial Resistances: The World's Next Pandemic On The WayIAEME PublicationNo ratings yet
- Antibiotic Resistance - A Global Issue of Concern: Rekha Bisht, Alok Katiyar, Rajat Singh, Piyush MittalDocument6 pagesAntibiotic Resistance - A Global Issue of Concern: Rekha Bisht, Alok Katiyar, Rajat Singh, Piyush MittalBramaNo ratings yet
- Artículo Resistant To Antibiotics. Alanis, 2005Document9 pagesArtículo Resistant To Antibiotics. Alanis, 2005JUAN ESTEBAN MONJE ROMERONo ratings yet
- AMR - Current Scenario and ChallangesDocument37 pagesAMR - Current Scenario and ChallangesShonit SharmaNo ratings yet
- Microbiology and Parasitology Presentation by W KakumuraDocument14 pagesMicrobiology and Parasitology Presentation by W KakumurahamiltonNo ratings yet
- Overview On Mechanisms of Antibacterial Resistance: Alemayehu Toma, Serawit DeynoDocument10 pagesOverview On Mechanisms of Antibacterial Resistance: Alemayehu Toma, Serawit DeynowaelNo ratings yet
- Bacterial Resistance To AntibioticsDocument37 pagesBacterial Resistance To Antibioticscristi69230% (1)
- Science Project That Takes Me So Long To Do It: What Is Antibiotics?Document4 pagesScience Project That Takes Me So Long To Do It: What Is Antibiotics?Vu Ba SonNo ratings yet
- Sabtu 2015Document9 pagesSabtu 2015Felicia BulaiNo ratings yet
- P RO JE CT: Theme:AntibioticDocument7 pagesP RO JE CT: Theme:AntibioticFijona KeloNo ratings yet
- Antibiotic Resistance: Microbiology: A Clinical Approach © Garland ScienceDocument40 pagesAntibiotic Resistance: Microbiology: A Clinical Approach © Garland ScienceAnonymous Ra09vhgLNo ratings yet
- Antimicrobial Resistance A Tale of The Past Becomes A Terrorfor The PresentDocument7 pagesAntimicrobial Resistance A Tale of The Past Becomes A Terrorfor The PresentdssgssNo ratings yet
- Antibióticos, Quimioterápicos e Resistência MicrobianaDocument54 pagesAntibióticos, Quimioterápicos e Resistência MicrobianaMarta BarbosaNo ratings yet
- Introduction To Pathology Infectious DiseasesDocument37 pagesIntroduction To Pathology Infectious DiseasesNirav PatelNo ratings yet
- An Introduction To Microbiology-An Overview2013Document34 pagesAn Introduction To Microbiology-An Overview2013Kelly YeowNo ratings yet
- PAIR in Vitro Activity of Pandan Pandanus Amaryllifolius Leaves CrudeDocument23 pagesPAIR in Vitro Activity of Pandan Pandanus Amaryllifolius Leaves CrudeMiftahurrachmahNo ratings yet
- Antimicrobial Resistance: The Indian ScenarioDocument14 pagesAntimicrobial Resistance: The Indian Scenariosungita_kNo ratings yet
- Name: Kiran Bhatti University: Liaquat University of Medical and Health Sciences. Pharm-D StudentDocument9 pagesName: Kiran Bhatti University: Liaquat University of Medical and Health Sciences. Pharm-D StudentPharmanic By Ruttaba FatimaNo ratings yet
- Antibiotic Resistance Thesis StatementDocument6 pagesAntibiotic Resistance Thesis Statementkatelogebellevue100% (2)
- Hello Bio InvestDocument16 pagesHello Bio InvestAadrica WaliaNo ratings yet
- Superbugs: Name Class: Section Roll NoDocument11 pagesSuperbugs: Name Class: Section Roll NoAshish ShendeNo ratings yet
- AntibioticsDocument8 pagesAntibioticsdocerick87No ratings yet
- Antiviral Agents: Unit - 2 Pharmaceutical Chemistry - I (Advanced Medicinal Chemistry) Topic: Antiviral AgentsDocument20 pagesAntiviral Agents: Unit - 2 Pharmaceutical Chemistry - I (Advanced Medicinal Chemistry) Topic: Antiviral AgentsGunjan Kalyani100% (1)
- Antibiotic Resistance and The New Antibiotic Agents: SV Want, A HolmesDocument7 pagesAntibiotic Resistance and The New Antibiotic Agents: SV Want, A Holmesudaysingh98No ratings yet
- Antimicrobial Susceptibility Testing (AST)Document41 pagesAntimicrobial Susceptibility Testing (AST)summiya100% (1)
- Lec 1 - IntroductionDocument54 pagesLec 1 - IntroductionpranavenNo ratings yet
- Antibiotic Resistance: 010/06/10/overuse-Of-Antibiotics-Spurs-Vicious-Cycle - AspxDocument11 pagesAntibiotic Resistance: 010/06/10/overuse-Of-Antibiotics-Spurs-Vicious-Cycle - AspxTaufiq ManeNo ratings yet
- The Role of Clinical Pharmacist in Combating Antibiotic ResistanceDocument4 pagesThe Role of Clinical Pharmacist in Combating Antibiotic ResistanceAnto BijuNo ratings yet
- BIOLOGY Practical File For Class 12Document12 pagesBIOLOGY Practical File For Class 12onlyaimiitNo ratings yet
- CNSH DPDocument6 pagesCNSH DPHồng HạnhNo ratings yet
- The State of Antibiotic Resistance in CambodiaDocument14 pagesThe State of Antibiotic Resistance in CambodiaMariah MenannoNo ratings yet
- Principles of Bacterial Infections and Anti-Infectives: Cause, Pathogenicity, and VirulenceDocument29 pagesPrinciples of Bacterial Infections and Anti-Infectives: Cause, Pathogenicity, and Virulencejheannie02100% (1)
- Big Chicken PDFDocument9 pagesBig Chicken PDFwamu885No ratings yet
- An Investegatory Project ReportDocument17 pagesAn Investegatory Project ReportKhushi kapseNo ratings yet
- Big Chicken CHPT 1 ExcerptDocument9 pagesBig Chicken CHPT 1 Excerptwamu885No ratings yet
- Antibiotic Resistance - Katia IskandarDocument50 pagesAntibiotic Resistance - Katia IskandarElvire AyoubNo ratings yet
- Week 2 Workshop 5 and 6Document6 pagesWeek 2 Workshop 5 and 6shlokNo ratings yet
- Antibiotic ResistanceDocument29 pagesAntibiotic ResistanceDian Aditama100% (1)
- Anti Infective DrugsDocument77 pagesAnti Infective DrugsAginaya ReinNo ratings yet
- Week Two: Biopharmaceuticals: History, Type, The Big Shift'Document26 pagesWeek Two: Biopharmaceuticals: History, Type, The Big Shift'ashish100% (1)
- The Microbial WorldDocument37 pagesThe Microbial WorldANIME SOLONo ratings yet
- How Microbes Rule The World?Document2 pagesHow Microbes Rule The World?tummalapalli venkateswara raoNo ratings yet
- Mrsa PP Microsoft PP PPT Final Without NCPDocument32 pagesMrsa PP Microsoft PP PPT Final Without NCPapi-355433171No ratings yet
- Radiology Icm IiDocument8 pagesRadiology Icm IijaneNo ratings yet
- Intratympanic Membrane Congenital CholesteatomaDocument3 pagesIntratympanic Membrane Congenital CholesteatomajaneNo ratings yet
- Antidepressants AntidepressantsDocument38 pagesAntidepressants AntidepressantsjaneNo ratings yet
- NIH Public Access: Delayed Antimicrobial Therapy Increases Mortality and Organ Dysfunction Duration in Pediatric SepsisDocument23 pagesNIH Public Access: Delayed Antimicrobial Therapy Increases Mortality and Organ Dysfunction Duration in Pediatric SepsisjaneNo ratings yet
- Medical Leadership Competency Framework: Landscape of HealthcareDocument15 pagesMedical Leadership Competency Framework: Landscape of HealthcarejaneNo ratings yet
- Substance Abuse Among Health Professionals: August 15, 2014Document25 pagesSubstance Abuse Among Health Professionals: August 15, 2014janeNo ratings yet
- By: Dr. Engelberta Sp. KJDocument14 pagesBy: Dr. Engelberta Sp. KJjaneNo ratings yet
- To Physiology, Homeostasis, and Body Temperature: V. Sutarmo SetiadjiDocument20 pagesTo Physiology, Homeostasis, and Body Temperature: V. Sutarmo SetiadjijaneNo ratings yet
- Lymphokines & Cytokines: Immunology & DiseaseDocument34 pagesLymphokines & Cytokines: Immunology & DiseasejaneNo ratings yet
- Itching, Redness of The SkinDocument21 pagesItching, Redness of The SkinjaneNo ratings yet
- JawsDocument78 pagesJawsjaneNo ratings yet
- COMMUNICATION With Other ProfessionalsDocument12 pagesCOMMUNICATION With Other ProfessionalsjaneNo ratings yet
- Transient Loss of Consciousness: History TakingDocument4 pagesTransient Loss of Consciousness: History TakingjaneNo ratings yet
- LibraryDocument1 pageLibraryjaneNo ratings yet
- STM Cels Lcture 1Document44 pagesSTM Cels Lcture 1janeNo ratings yet
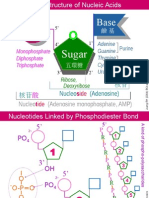
- NA01 StructureDocument5 pagesNA01 StructurejaneNo ratings yet
- EPS 001 Incubating and Hatching Eggs1 PDFDocument13 pagesEPS 001 Incubating and Hatching Eggs1 PDFsanthoshNo ratings yet
- X Extra-NuclearDocument11 pagesX Extra-Nuclearnsjunnarkar100% (1)
- Curriculum Vitae: G.SethuramanDocument4 pagesCurriculum Vitae: G.SethuramanSethuNo ratings yet
- 13-1: The Genetic Material: Frederick Griffith's Experiment - TransformationDocument7 pages13-1: The Genetic Material: Frederick Griffith's Experiment - Transformationapi-233187566No ratings yet
- Stress BustingDocument24 pagesStress BustingMarianne ChristieNo ratings yet
- Quiz Chapter 62 63Document2 pagesQuiz Chapter 62 63Amelie AvenidoNo ratings yet
- Taurine: S. Oja and Pirjo KontroDocument2 pagesTaurine: S. Oja and Pirjo KontroericNo ratings yet
- Eye Cancer - Stages and Grades - 2015-09-01Document7 pagesEye Cancer - Stages and Grades - 2015-09-01Ruslan KamilNo ratings yet
- Failure To ThriveDocument53 pagesFailure To Thrivesciatic100% (2)
- Muhs 2K17 PDFDocument24 pagesMuhs 2K17 PDFJenniferNo ratings yet
- Rare Blood Groups - Characterisation and Clinical SignificanceDocument38 pagesRare Blood Groups - Characterisation and Clinical SignificanceZaira KimNo ratings yet
- 9700 s13 QP 11Document16 pages9700 s13 QP 11Joyce GohNo ratings yet
- Harpers Illustrated Biochemistry 32Th Ed 32Nd Edition Peter J Kennelly Full ChapterDocument67 pagesHarpers Illustrated Biochemistry 32Th Ed 32Nd Edition Peter J Kennelly Full Chaptersally.kimberlin556No ratings yet
- Drug Addiction Is A State of PeriodicDocument8 pagesDrug Addiction Is A State of PeriodicBastab DeyNo ratings yet
- Etiopathogenesis of Diabetes MellitusDocument35 pagesEtiopathogenesis of Diabetes MellitusironNo ratings yet
- Intro To Genetics WebQuestDocument3 pagesIntro To Genetics WebQuestFRANKLIN Ofori100% (1)
- ch01 PDFDocument5 pagesch01 PDFHugsNo ratings yet
- PCOG - I COurse ScheduleDocument2 pagesPCOG - I COurse ScheduleAmjad KhanNo ratings yet
- 6 MUTATION LatestDocument67 pages6 MUTATION LatesthashimNo ratings yet
- Disabilities Research Paper - Morgen GreifDocument10 pagesDisabilities Research Paper - Morgen Greifapi-604606576No ratings yet
- S. S. Jain Subodh PG (Autonomous) College Rambagh Circle, Jaipur - 302004Document43 pagesS. S. Jain Subodh PG (Autonomous) College Rambagh Circle, Jaipur - 302004rahulvikiNo ratings yet
- Genetics Problem SetDocument6 pagesGenetics Problem SetKunvarNo ratings yet
- Zab Mohsenifar, Guy W. Soo Hoo Lung Biology in Health & Disease Volume 213 Practical Pulmonary and Critical Care Medicine Respiratory Failure PDFDocument444 pagesZab Mohsenifar, Guy W. Soo Hoo Lung Biology in Health & Disease Volume 213 Practical Pulmonary and Critical Care Medicine Respiratory Failure PDFAnca Dumitru50% (2)
- Animal Testing (Black Mamba)Document3 pagesAnimal Testing (Black Mamba)Robespade El PistoleroNo ratings yet
- Detailed EoT Coverage 9 ADVDocument50 pagesDetailed EoT Coverage 9 ADVNKANo ratings yet
- Molecular Techniques For Detection, Species DifferentiationDocument43 pagesMolecular Techniques For Detection, Species DifferentiationUziel Castillo VelazquezNo ratings yet
- What Are The Different Types of BiochipDocument2 pagesWhat Are The Different Types of Biochipajrai07No ratings yet
- Medical TerminologyDocument10 pagesMedical Terminologyfreedomx0a100% (2)
- Humor, Laughter, and AgingDocument2 pagesHumor, Laughter, and AgingGordon LoganNo ratings yet
- Control Flebotominos PyvDocument37 pagesControl Flebotominos PyvDaniel Alfredo Galindo ChoqueNo ratings yet
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsFrom EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsRating: 4.5 out of 5 stars4.5/5 (6)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Fatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthFrom EverandFatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthRating: 4 out of 5 stars4/5 (7)
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthFrom EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthNo ratings yet
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- Summary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedNo ratings yet
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryFrom EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryRating: 4 out of 5 stars4/5 (6)
- Sickening: How Big Pharma Broke American Health Care and How We Can Repair ItFrom EverandSickening: How Big Pharma Broke American Health Care and How We Can Repair ItRating: 4 out of 5 stars4/5 (9)
- The Hair Color Mix Book: More Than 150 Recipes for Salon-Perfect Color at HomeFrom EverandThe Hair Color Mix Book: More Than 150 Recipes for Salon-Perfect Color at HomeRating: 3.5 out of 5 stars3.5/5 (7)
- The Inescapable Immune Escape PandemicFrom EverandThe Inescapable Immune Escape PandemicRating: 5 out of 5 stars5/5 (1)
- War on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicFrom EverandWar on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicRating: 4 out of 5 stars4/5 (7)
- Microbiological Quality of FoodsFrom EverandMicrobiological Quality of FoodsL SlanetzNo ratings yet
- Profiles of the Vaccine-Injured: "A Lifetime Price to Pay"From EverandProfiles of the Vaccine-Injured: "A Lifetime Price to Pay"Rating: 3.5 out of 5 stars3.5/5 (3)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceFrom EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceRating: 4.5 out of 5 stars4.5/5 (15)
- Vaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadFrom EverandVaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadRating: 4.5 out of 5 stars4.5/5 (3)
- Epidemics and Society: From the Black Death to the PresentFrom EverandEpidemics and Society: From the Black Death to the PresentRating: 4.5 out of 5 stars4.5/5 (9)
- Arthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefFrom EverandArthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefNo ratings yet
- Make America Healthy Again: How Bad Behavior and Big Government Caused a Trillion-Dollar CrisisFrom EverandMake America Healthy Again: How Bad Behavior and Big Government Caused a Trillion-Dollar CrisisNo ratings yet
- The Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusFrom EverandThe Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusRating: 4.5 out of 5 stars4.5/5 (10)
- The Gut-loving Cookbook: Over 65 deliciously simple, gut-friendly recipes from The Gut StuffFrom EverandThe Gut-loving Cookbook: Over 65 deliciously simple, gut-friendly recipes from The Gut StuffNo ratings yet
- Panic Attack: Playing Politics with Science in the Fight Against COVID-19From EverandPanic Attack: Playing Politics with Science in the Fight Against COVID-19Rating: 4.5 out of 5 stars4.5/5 (10)