You might also like
- Hanna Oberg: Get Lean. Stay HealthyDocument22 pagesHanna Oberg: Get Lean. Stay HealthyMallorie Mayer88% (49)
- NLE Compilation 1Document67 pagesNLE Compilation 1blazegomez91% (34)
- (Book 1) : Career Paths: Physiotherapy - GlossaryDocument15 pages(Book 1) : Career Paths: Physiotherapy - Glossarygab77No ratings yet
- Brachial Plexus InjuryDocument21 pagesBrachial Plexus InjurySemi IqbalNo ratings yet
- Capsular Pattern of Joint - For MergeDocument17 pagesCapsular Pattern of Joint - For MergeSiva ShanmugamNo ratings yet
- Clinical Biomechanics of Gait: OutlineDocument7 pagesClinical Biomechanics of Gait: Outlinechacho1971100% (1)
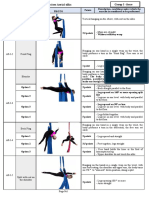
- Appendix 1 Compulsory Exercises Aerial Silk Eng 2018Document23 pagesAppendix 1 Compulsory Exercises Aerial Silk Eng 2018tito1628100% (6)
- Cyriax - Spine: by DR. Akshay A. Chougule (PT) Orthopaedic Manual TherapistDocument44 pagesCyriax - Spine: by DR. Akshay A. Chougule (PT) Orthopaedic Manual TherapistAishwarya Shah100% (1)
- Ataxias Neuro Condition DetailedDocument80 pagesAtaxias Neuro Condition DetailedMikail AtiyehNo ratings yet
- Electrotherapy: DR Ramaiah Choudhary PhysiotherapistDocument13 pagesElectrotherapy: DR Ramaiah Choudhary Physiotherapistvenkata ramakrishnaiahNo ratings yet
- Shoulder ComplexDocument14 pagesShoulder Complexbhavesh jain100% (5)
- Thorax and Chest WallDocument6 pagesThorax and Chest WallDale P. PolvorosaNo ratings yet
- Tx3: Bobath'S Neurodevelopmental Treatment: PT Applications Team DLSMHSI CRS PT Department AY 2018-2019Document4 pagesTx3: Bobath'S Neurodevelopmental Treatment: PT Applications Team DLSMHSI CRS PT Department AY 2018-2019Pauline JaleaNo ratings yet
- DiathermyDocument55 pagesDiathermyHaniya KhanNo ratings yet
- Coordination AssessmentDocument30 pagesCoordination AssessmentBhawna PalNo ratings yet
- Lung SurgeriesDocument43 pagesLung SurgeriesSereinNo ratings yet
- Vojta Therapy: Reflex Creeping in A Prone Lying Position and Reflex Rolling From A Supine and Side LyingDocument7 pagesVojta Therapy: Reflex Creeping in A Prone Lying Position and Reflex Rolling From A Supine and Side LyingSonali SoumyashreeNo ratings yet
- Brunstorm'sDocument19 pagesBrunstorm'sHARSH 23 (Jalu)No ratings yet
- PNF FullDocument46 pagesPNF FullHUZAIFA YAMAAN100% (1)
- Special Tests For WristDocument13 pagesSpecial Tests For WristSaif Ahmed LariNo ratings yet
- Brunnstrom ApproachDocument26 pagesBrunnstrom ApproachMohaChebiNo ratings yet
- Biomechanics of Peripheral and Spinal Nerve RootsDocument86 pagesBiomechanics of Peripheral and Spinal Nerve RootsJawad HassanNo ratings yet
- BobathDocument28 pagesBobathSaba SamimNo ratings yet
- Bicipital TendonitisDocument2 pagesBicipital TendonitisJ Cheung100% (2)
- Cervical RibDocument15 pagesCervical RibArko duttaNo ratings yet
- Neuro-Coordination Umair PTDocument20 pagesNeuro-Coordination Umair PTFatima SeharNo ratings yet
- ShoulderDocument51 pagesShoulderIts LaraNo ratings yet
- Chest Physical TherapyDocument28 pagesChest Physical TherapyJulia SalvioNo ratings yet
- Introduction To MovementsDocument42 pagesIntroduction To MovementsRamalingam KanagarajNo ratings yet
- Rood ApproachDocument36 pagesRood Approachshemjaz100% (1)
- Dysphagia ManagementDocument21 pagesDysphagia ManagementSooraj A. O.100% (1)
- Faradic Foot BathDocument16 pagesFaradic Foot BathMaansi Gupta100% (1)
- Hip Complex BioDocument18 pagesHip Complex BioVijay PradeepNo ratings yet
- Short WaveDocument31 pagesShort WaveDharmesh MaheshwariNo ratings yet
- The Wrist ComplexDocument35 pagesThe Wrist ComplexKeshav Singhmaar AryaNo ratings yet
- Neurological ExaminationDocument13 pagesNeurological Examinationsaveetha purushothamanNo ratings yet
- Movement Disorders Types - Mayo ClinicDocument1 pageMovement Disorders Types - Mayo ClinicdrrajmptnNo ratings yet
- The Elbow ComplexDocument12 pagesThe Elbow ComplextafelaNo ratings yet
- Chap 7-BiofeedbackDocument32 pagesChap 7-Biofeedbackaarya12No ratings yet
- Brunnstrom ApproachDocument33 pagesBrunnstrom ApproachAISHWARYA SWAMINATHANNo ratings yet
- 6 Brunnstrom Approach Part 4Document23 pages6 Brunnstrom Approach Part 4johnclyde fantone100% (1)
- Coordination Exercise 3Document16 pagesCoordination Exercise 3Ella CooperNo ratings yet
- Neuro Developmental Treatment (NDT) Techniques: HistoryDocument3 pagesNeuro Developmental Treatment (NDT) Techniques: HistoryGafencu SergiuNo ratings yet
- Periarthritis Shoulder By: DR - Sindhu.MPT (Ortho)Document39 pagesPeriarthritis Shoulder By: DR - Sindhu.MPT (Ortho)Michael Selvaraj100% (1)
- 4 - Therapeutic Effects of Low Frequency Currents On TissuesIVDocument52 pages4 - Therapeutic Effects of Low Frequency Currents On TissuesIVhuxley2378No ratings yet
- Gait AnalysisDocument6 pagesGait AnalysisryankelsallNo ratings yet
- Physiotherapy For PoliomyelitisDocument16 pagesPhysiotherapy For Poliomyelitisabdalsucs100% (1)
- I. Etiology Primary Adhesive Capsulitis Secondary Adhesive CapsulitisDocument8 pagesI. Etiology Primary Adhesive Capsulitis Secondary Adhesive CapsulitisVanessa Yvonne Gurtiza100% (1)
- Tennis Elbow PDFDocument2 pagesTennis Elbow PDFSabau PetreNo ratings yet
- Articular Neurophysiology: Presented by - Yogesh VyasDocument15 pagesArticular Neurophysiology: Presented by - Yogesh VyasvictoryvelavaNo ratings yet
- Brachial Plexus InjuriesDocument64 pagesBrachial Plexus Injuriesprashanth naikNo ratings yet
- Elbow Special TestDocument4 pagesElbow Special TestEllaiza Astacaan100% (1)
- Chapter # 4: Physical Assessment As A Screening ToolDocument89 pagesChapter # 4: Physical Assessment As A Screening Toolmuhammad awaisNo ratings yet
- Program - B.P.T - Second Year: 2021 - 2022/ Lecture No - 10 (08.02.22)Document23 pagesProgram - B.P.T - Second Year: 2021 - 2022/ Lecture No - 10 (08.02.22)Katy PerrieNo ratings yet
- Biomechanics of The Vertebral ColumnDocument44 pagesBiomechanics of The Vertebral ColumnVijay PradeepNo ratings yet
- Spinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PuneDocument43 pagesSpinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PunePraneetha NouduriNo ratings yet
- Faradic Foot Bath & Faradism Under PressureDocument6 pagesFaradic Foot Bath & Faradism Under PressureNamrathaThalatoti ywSSAmHsULNo ratings yet
- Rehabilitation Engineering Fact Sheet PDFDocument2 pagesRehabilitation Engineering Fact Sheet PDFYahya AlkamaliNo ratings yet
- Spinal Cord InjuryDocument39 pagesSpinal Cord InjuryrahatNo ratings yet
- Gait Analysis PresentationDocument41 pagesGait Analysis PresentationKýñg ButlerNo ratings yet
- Abnormal Gait: Department of Physical Therapy New York UniversityDocument79 pagesAbnormal Gait: Department of Physical Therapy New York UniversityAlok_Singh_9371No ratings yet
- DR Sapna Ali Khan (PT) DPT, MSPTDocument32 pagesDR Sapna Ali Khan (PT) DPT, MSPTCHANGEZ KHAN SARDARNo ratings yet
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- LCB Surgical Technique - 2022 Update v3Document24 pagesLCB Surgical Technique - 2022 Update v3Samuel SalvadorNo ratings yet
- The Four Phases of The Long Jump:, ,, Approach:: SpeedDocument4 pagesThe Four Phases of The Long Jump:, ,, Approach:: SpeedCiprian CorneaNo ratings yet
- Positioning and Moving of Hemiplegic Pt. Bed Mobility ExercisesDocument133 pagesPositioning and Moving of Hemiplegic Pt. Bed Mobility Exercisesktin17100% (1)
- Medical Mnemonics 4 PrintDocument65 pagesMedical Mnemonics 4 Printanne0521100% (1)
- Ukite 2009Document69 pagesUkite 2009pikacu196100% (1)
- Test of Gross Motor Development Test Administration and Scoring Procedures Time RequirementsDocument8 pagesTest of Gross Motor Development Test Administration and Scoring Procedures Time RequirementsLIM JUN YAN MoeNo ratings yet
- Motor Control Motor LearningDocument56 pagesMotor Control Motor LearningJune EpeNo ratings yet
- Pdhpe HSC Core 2Document10 pagesPdhpe HSC Core 2Toby FergusonNo ratings yet
- Fgcu Aquila 0011 Castellanos Motion AnalysisDocument9 pagesFgcu Aquila 0011 Castellanos Motion AnalysisYasser EidNo ratings yet
- OSCE Surgery BlockDocument31 pagesOSCE Surgery Blockmyat25100% (6)
- Active Jacquelyn - Get Stretchy 1.0Document17 pagesActive Jacquelyn - Get Stretchy 1.0Ashita Sharma100% (1)
- Glasgocoma ScaleDocument35 pagesGlasgocoma Scalepop lopNo ratings yet
- Brunnstrom'S Movement Therapy in HemiplegiaDocument9 pagesBrunnstrom'S Movement Therapy in HemiplegiaLall JingerppangNo ratings yet
- NKT FlowChart - PDF Version 1 PDFDocument2 pagesNKT FlowChart - PDF Version 1 PDFJay SarkNo ratings yet
- MD 1st Year Rachna Sharir Shariropkrama 18-05-2020Document42 pagesMD 1st Year Rachna Sharir Shariropkrama 18-05-2020Dr.Mahesh kumar GuptaNo ratings yet
- Crawling Exercise: Dr. Hiral Katakia MPT (Neuro)Document20 pagesCrawling Exercise: Dr. Hiral Katakia MPT (Neuro)Rohan LAl100% (3)
- Aao Sport 2016Document84 pagesAao Sport 2016Anonymous 43mqs5pElf100% (3)
- Chronic Shoulder Pain - Part I Evaluation & DiagnosisDocument8 pagesChronic Shoulder Pain - Part I Evaluation & Diagnosisgozjasa100% (1)
- Neurological Examination in Psychiatry: Abid Rizvi Junior Resident 3 Department of PsychiatryDocument149 pagesNeurological Examination in Psychiatry: Abid Rizvi Junior Resident 3 Department of PsychiatryMohammed ArarNo ratings yet
- HCI College Physical Fitness Test Info Kit For Students 2019 PDFDocument47 pagesHCI College Physical Fitness Test Info Kit For Students 2019 PDFANDRE LIM BU YUN Year14No ratings yet
- Afo Desain Dan KomponenDocument18 pagesAfo Desain Dan KomponenNafisah Bochil100% (1)
- Camptodactyly: Amalia Irsha Adhari (1506668510) Eldesta Nisa Nabila (1406642233)Document38 pagesCamptodactyly: Amalia Irsha Adhari (1506668510) Eldesta Nisa Nabila (1406642233)Amalia IrshaNo ratings yet
- Swing ThoughtsDocument9 pagesSwing Thoughtsodic200250% (2)
- Thai Foot Reflexology With The Wooden Stick Autor Heath & Nicole ReedDocument17 pagesThai Foot Reflexology With The Wooden Stick Autor Heath & Nicole ReedAlvydas VitkauskasNo ratings yet
- Why Are Cervicals Adjust Prone or Seated in GonsteadDocument16 pagesWhy Are Cervicals Adjust Prone or Seated in Gonsteadgonsteadtruth100% (3)